Anatomical Overview
A supracondylar fracture of the humerus occurs at the junction between the humeral shaft and the humeral condyles. The anatomical predisposition for this injury is attributed to the 30°–50° anterior inclination angle between the axis of the humeral shaft and the axis of the humeral condyles. Critical neurovascular structures, including the brachial artery and median nerve, traverse the medial and anterior aspects of the humeral condyles. These structures lie superficial to the robust bicipital aponeurosis and posterior to the humerus, rendering them vulnerable to injury during fractures. Additionally, the ulnar nerve courses posteromedially, and the radial nerve lies laterally near the condyles, both of which may be compromised by lateral displacement of the fracture fragments. In children, the distal humerus contains an epiphyseal plate. Fractures involving the physeal line may disrupt epiphyseal growth, often resulting in cubitus varus or valgus deformities. Supracondylar fractures predominantly affect children under 10 years of age and are classified into flexion and extension types based on the direction of force and displacement, with the extension type accounting for approximately 97% of cases.
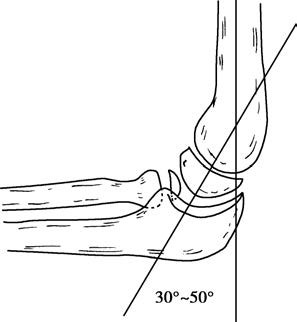
Figure 1 Anterior inclination angle between the humeral shaft and humeral condyles
To be continued