Intestinal intussusception refers to the invagination of one segment of the intestine into the lumen of an adjacent intestinal segment. It is more commonly observed in infants and young children, while adult cases are rare but exhibit distinct characteristics.
Etiology and Types
Primary intussusception occurs predominantly in infants and young children and is primarily due to disrupted normal bowel peristaltic rhythm. The dysregulation of bowel motility is often associated with changes in food consistency. Secondary intussusception is more commonly seen in adults and may involve anatomical factors, such as excessive mobility of the cecum. Other physical factors, including organic lesions within the intestinal lumen or wall (such as intestinal polyps or tumors), can also disrupt peristalsis. In these cases, the vigorous peristalsis of the proximal segment may propel both the pathological lesion and the adjacent intestinal segment into the distal bowel.
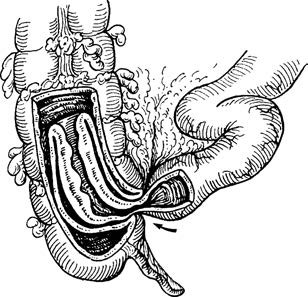
Figure 1 Ileocecal intussusception
Intussusception can be categorized according to the involved intestinal segments, including small intestine-to-small intestine, small intestine-to-colon, and colon-to-colon types. In children, ileocolic intussusception is the most common form. Structurally, intussusception involves three layers: the outer sheath (the intussuscipiens), the middle return layer, and the inner entering layer, with the latter two collectively referred to as the intussusceptum. The mesentery associated with the intussusceptum also invaginates, leading to intestinal obstruction and mesenteric vascular compression, which can result in strangulation and necrosis of the affected bowel segment.
Clinical Manifestations
The three classic symptoms of intussusception are abdominal pain, blood in the stool, and an abdominal mass. Symptoms often present as sudden onset of severe, intermittent abdominal pain. Infants and young children may exhibit episodes of crying and distress, followed by calm intervals. This may be accompanied by vomiting and red jelly-like stools. Abdominal palpation often reveals a sausage-shaped, smooth, slightly mobile, and tender mass, which is typically located in the upper right quadrant near the umbilicus. In addition, palpation of the lower right abdomen may reveal a sensation of emptiness. As the condition progresses, signs of intestinal obstruction, such as abdominal distension, gradually appear. A barium enema X-ray or CT scan can aid in diagnosis.
Apart from acute intussusception, chronic recurrent intussusception may also occur, particularly in adults. This condition is often associated with pathological factors, such as intestinal polyps, tumors, or diverticula. It typically presents as incomplete obstruction with milder symptoms, including intermittent abdominal pain, while significant bleeding is uncommon. Intussusception in these cases often resolves spontaneously, and diagnostic tests performed after resolution may yield negative results.
Treatment
Air or barium enema can serve as both a diagnostic and therapeutic approach, particularly for early cases of ileocecal or colonic intussusception. Air pressure is generally started at 60 mmHg and introduced into the colon via a rectal catheter under X-ray fluoroscopy. After diagnosis is confirmed, the pressure may be gradually increased to approximately 80 mmHg until successful reduction of the intussusception is achieved.
Surgical intervention should be considered when reduction cannot be achieved, the duration of symptoms exceeds 48 hours, bowel necrosis is suspected, or signs of peritoneal irritation or systemic deterioration occur following enema reduction. Preoperative correction of dehydration or shock is essential. During surgery, if the intestine is found to be viable, gentle manual reduction may be performed. For cases with severe intestinal wall damage or confirmed bowel necrosis, resection of the affected segment followed by anastomosis may be necessary. In severely ill pediatric patients, necrotic bowel segments may be resected with external diversion of the intestinal stumps, with bowel anastomosis deferred to a second-stage procedure.
In adults, intussusception is often associated with underlying pathological causes, and surgery is generally recommended.