Adhesive intestinal obstruction is the most common type of intestinal obstruction, accounting for approximately 40% to 60% of cases.
Etiology and Pathology
Intestinal adhesions and intra-abdominal adhesive bands can be categorized as congenital or acquired. Congenital causes are relatively rare and may result from developmental abnormalities or meconium peritonitis. Acquired causes are more common and are typically related to abdominal surgeries, inflammation, trauma, bleeding, foreign bodies, and other factors. Among these, postoperative adhesive intestinal obstruction is the most frequent in clinical settings. Not all intestinal adhesions lead to intestinal obstruction. Adhesive intestinal obstruction typically occurs in the small bowel, with involvement of the colon being rare. Several types of intestinal obstruction may result from adhesions.
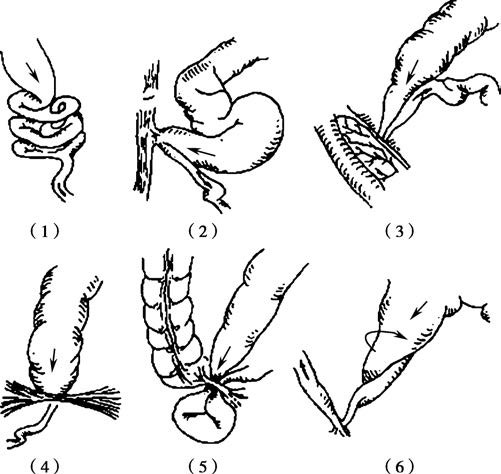
Figure 1 Various types of adhesive intestinal obstruction
1, Intestinal loops adhered into a mass
2, Adherence and kinking at the abdominal wall
3, Adherence and kinking at the mesentery
4, Adhesive bands
5, Adhesive internal hernia
6, Adhesions causing angulation or volvulus
Diagnosis
Diagnosis is generally not difficult when considering the medical history, clinical symptoms, and imaging findings. When obstruction symptoms occur early after surgery (within 5 to 7 days), differentiation must be made between adhesive intestinal obstruction and postoperative ileus caused by impaired bowel motility during the recovery period. The latter condition is associated with postoperative inflammatory reactions within the bowel in addition to adhesions, leading to both luminal obstruction and local dysmotility induced by inflammation.
Prevention
Efforts during abdominal surgeries to minimize tissue injury and inflammatory response can help prevent intra-abdominal adhesions. While adhesions may not be entirely avoidable, several measures can reduce their occurrence:
- Removing particles such as starch or talc from gloves and ensuring no suture remnants, cotton fibers, or other foreign bodies remain in the abdominal cavity to reduce granulation tissue formation.
- Minimizing ischemic tissue and avoiding ligation of large tissue segments.
- Maintaining aseptic technique to reduce inflammatory exudation.
- Protecting the serosal surface of the bowel to prevent injury and desiccation.
- Irrigating the abdominal cavity to remove blood and fluid accumulation and placing appropriate drainage when necessary.
- Promptly addressing intra-abdominal inflammatory conditions to prevent their spread.
Postoperative early mobilization and efforts to restore bowel motility promptly also play a role in reducing the formation of adhesions.
Treatment
The general treatment principles for intestinal obstruction also apply to adhesive intestinal obstruction. Non-surgical management may be attempted initially for simple intestinal obstruction, while strangulated or complete obstruction typically requires surgical intervention. For patients experiencing recurrent episodes, surgical treatment can be considered depending on the clinical situation. Although adhesions may still form after surgery, surgical intervention remains an effective method when non-surgical approaches fail to resolve the obstruction.
The choice of surgical technique depends on the specific characteristics of the adhesion:
- Simple transection and adhesion lysis are appropriate for localized adhesive bands or small patches of adhesions.
- For tightly adherent clusters of intestinal loops that are difficult to separate, resection of the affected segment of bowel with primary anastomosis may be necessary.
- In special cases, side-to-side anastomosis between the proximal and distal segments of the obstructed bowel can be performed as a bypass surgery.
- To reduce the risk of postoperative recurrence of adhesive intestinal obstruction, particularly after extensive intra-abdominal adhesion lysis, intestinal splinting techniques may be employed. This method involves arranging the intestinal loops in an orderly manner to minimize the likelihood of obstruction caused by re-adhesion.