Thromboangiitis obliterans (TAO), also known as Buerger's disease, is a chronic, segmental, and recurring inflammatory occlusive condition affecting blood vessels. It primarily involves the small and medium-sized arteries and veins of the extremities, with a predilection for the lower limbs. The disease most commonly occurs in young adult males.
Etiology and Pathology
The exact cause remains unclear, but contributing factors can be categorized as follows:
- External Factors: Smoking (active or passive), exposure to cold and damp environments, chronic injury, and infections.
- Internal Factors: Dysregulated immune function, imbalance of sex hormones and prostaglandins, and genetic predisposition. Among these, active or passive smoking is considered a significant risk factor for the onset and progression of the disease.
The pathological features of TAO are as follows:
- It typically begins in the arteries and subsequently involves veins, progressing from distal to proximal segments in a segmental distribution, with relatively normal vessels between affected segments.
- In the active phase, there is non-suppurative inflammation involving all layers of the affected vessels, with thrombosis occluding the lumen.
- In later stages, inflammation subsides, thrombi undergo organization, and new capillaries form.
Although collateral circulation gradually develops, it is often insufficient to compensate for the ischemia, leading to ischemic changes in the nerves, muscles, and bones.
Clinical Manifestations
The disease has an insidious onset and progresses slowly, with symptoms becoming more pronounced and severe after multiple episodes. The main clinical features include:
- Cold Sensitivity and Skin Temperature Changes: The affected limb often feels cold, with reduced skin temperature, pallor, or cyanosis.
- Sensory Abnormalities and Pain: Early pain arises due to inflammation of the vessel wall irritating peripheral nerves. Later, ischemic pain occurs due to arterial occlusion, presenting as intermittent claudication or rest pain.
- Trophic Changes: Chronic ischemia results in tissue nutritional deficiencies, and severe cases may lead to ischemic ulcers or gangrene at the distal limb.
- Diminished or Absent Pulses: Pulses in the distal arteries of the affected limb are weakened or absent.
- Recurrent Migratory Superficial Thrombophlebitis: This may occur before or during disease progression.
Diagnostic Evaluation
The key diagnostic criteria include:
- Most patients are young adult males, often with a history of smoking.
- The affected limb exhibits varying degrees of ischemic symptoms.
- A history of migratory superficial thrombophlebitis is present.
- Pulses in the dorsalis pedis artery or posterior tibial artery are diminished or absent in the affected limb.
- Common high-risk factors for atherosclerosis, such as hypertension, hyperlipidemia, and diabetes mellitus, are typically absent.
Both general and specialized diagnostic tests used for arteriosclerosis obliterans are applicable to TAO. Arteriography is crucial in determining the location, severity, extent of arterial obstruction, and status of collateral circulation. Imaging findings typically show segmental stenosis or occlusion of the small and medium arteries in the affected limb. The tibial arteries (anterior and posterior tibial arteries, as well as peroneal artery) are commonly involved, with one to all three arteries affected. In later stages, the popliteal and femoral arteries may also be involved. Collateral arteries, often described as fine corkscrew-like vessels extending along occluded arteries, are considered a hallmark of TAO. Differentiation from arteriosclerosis obliterans and non-vascular causes of lower limb pain, as well as other arterial diseases, is essential (see Table 1 for diagnostic distinctions).
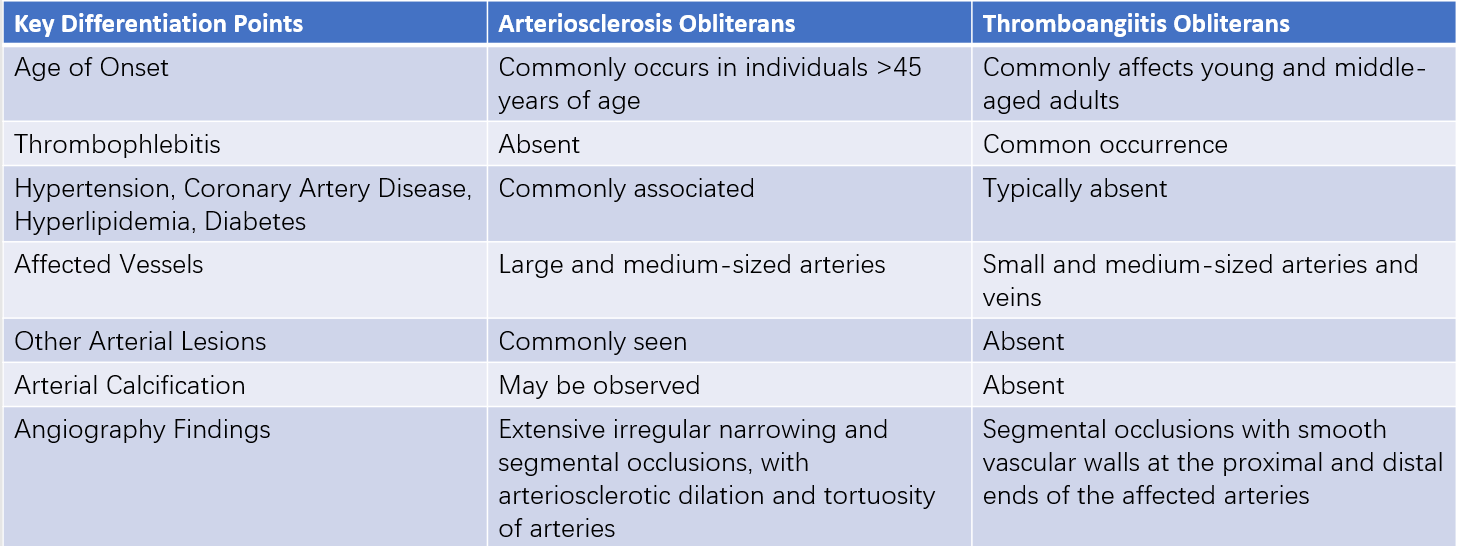
Table 1 Differentiation between arteriosclerosis obliterans and thromboangiitis obliterans
Prevention and Treatment
The management principles focus on preventing disease progression, improving blood circulation in the affected limbs, and promoting symptomatic relief.
General Measures
Absolute smoking cessation is required. Avoidance of cold and damp conditions, as well as protection from trauma, is recommended. Heat therapy is generally avoided to prevent increasing oxygen demand in tissues, which may worsen symptoms. Analgesics may be used for severe pain, with caution exercised regarding addictive medications. Moderate exercise for the affected limb can help promote collateral circulation.
Non-Surgical Treatment
Treatment includes antiplatelet aggregation and vasodilator drugs, as well as hyperbaric oxygen therapy.
Surgical Treatment
The aim is to reconstruct arterial flow, enhance blood supply, and alleviate ischemic consequences. Bypass grafting can be performed if there is a patent arterial inflow and outflow path near the occluded segment. However, due to the involvement of small and medium-sized arteries, suitable outflow tracts are often lacking, making bypass surgery less feasible. Techniques such as venous arterialization and percutaneous transluminal angioplasty (PTA) may provide limited benefits for certain patients. Overall, compared to arteriosclerosis obliterans, conventional revascularization surgeries are less effective in managing TAO.
For patients with ischemic ulcers or gangrene in distal limbs, wound care is critical, with the administration of appropriate antibiotics. Amputation should be considered when irreversible necrosis has occurred.
Other Treatments
Emerging therapies such as cell-based treatments show promise. Autologous stem cells can secrete cytokines and promote angiogenesis in the affected limbs, improving blood supply and offering a potentially favorable outcome.