A neck mass can be a manifestation of diseases originating in the neck or in other parts of the body and is commonly seen in clinical practice. The causes include tumors, inflammation, and congenital anomalies. Due to the significant proportion of malignant tumors, the differential diagnosis of a neck mass holds critical clinical importance.
Tumors
Primary Tumors
Benign tumors include thyroid adenomas, hemangiomas, and others. Malignant tumors include thyroid carcinoma, malignant lymphoma, salivary gland cancer, and more.
Metastatic Tumors
The primary lesions are often located in regions such as the oral cavity, nasopharynx, thyroid, lungs, mediastinum, breasts, gastrointestinal tract, and pancreas.
Inflammation
Examples include acute and chronic lymphadenitis, tuberculous lymphadenitis, and soft tissue infections.
Congenital Anomalies
Conditions such as thyroglossal duct cysts or fistulas, thymopharyngeal duct cysts or fistulas, cystic lymphangiomas (also known as cystic hygromas), and dermoid cysts are included.
Establishing a definitive diagnosis requires a comprehensive analysis based on the location of the mass, medical history, and findings from physical examinations. When necessary, fine-needle aspiration or excisional biopsy of the mass may be performed.
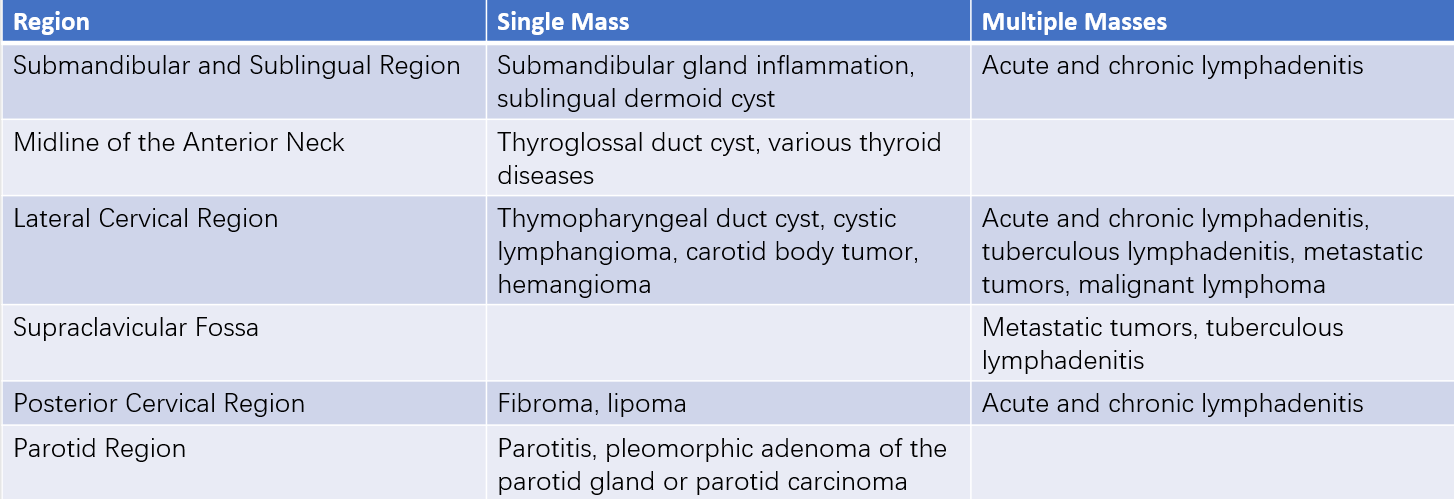
Table 1 Common masses in different cervical regions
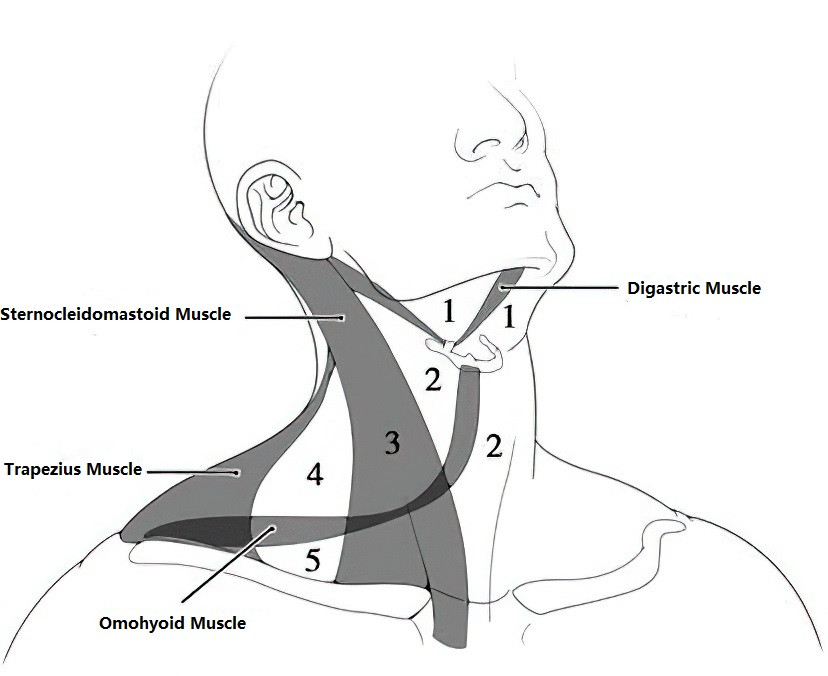
Figure 1 Anatomical divisions of the neck
Anterior Cervical Region:
1, Submandibular and sublingual region
2, Midline of the anterior neck
Lateral Cervical Region:
3, Sternocleidomastoid muscle region
4, Omohyoid and trapezius region
5, Supraclavicular fossa
Common Types of Neck Masses
Chronic Lymphadenitis
This condition is often secondary to inflammatory lesions in the head, face, or neck. Enlarged lymph nodes are scattered in the lateral cervical or submandibular areas. When searching for the primary lesion, particular attention should be given to the lymphatic drainage area of the enlarged lymph nodes. Distinguishing between chronic lymphadenitis and a malignant condition may require excisional biopsy of the enlarged lymph node for pathological examination.
Thyroid Diseases
Details are discussed under the category of thyroid diseases.
Metastatic Tumors
Metastatic tumors account for the second-highest incidence of neck masses after chronic lymphadenitis and thyroid diseases. The primary cancer site for most metastatic cervical lymphadenopathy cases (85%) originates in the head and neck region, particularly nasopharyngeal carcinoma and thyroid carcinoma. For metastatic lymph nodes in the supraclavicular fossa, the primary lesions are often in the thoracoabdominal region, with gastrointestinal and pancreatic tumors frequently spreading to the left supraclavicular lymph nodes via the thoracic duct.
Malignant Lymphoma
Malignant lymphoma, including Hodgkin’s lymphoma and non-Hodgkin’s lymphoma, arises from malignant proliferation of lymphoid tissue. It is most commonly observed in young and middle-aged men. Enlarged lymph nodes typically appear first in one or both lateral cervical regions, grow rapidly, and may adhere together to form a cluster. Confirmation of the diagnosis requires pathological examination of the lymph nodes.
Thyroglossal Duct Cyst
This congenital anomaly is related to the development of the thyroid gland. During the embryonic stage, the thyroid gland originates from the caudal end of the thyroglossal duct, which extends from the floor of the mouth to the neck. Normally, the thyroglossal duct obliterates spontaneously by approximately the sixth week of fetal development. Incomplete regression of the duct can lead to the formation of a congenital cyst, which, if infected and ruptured, may result in a thyroglossal fistula.
This condition is most commonly identified in children under 15 years of age, with a male-to-female ratio of 2:1. It manifests as a well-defined, round mass with a diameter of 1–2 cm, located in the midline of the anterior neck below the hyoid bone. The surface is smooth, cystic in nature, and the mass moves up and down with tongue movement.
Treatment involves complete excision of the cyst or fistula. Resection includes part of the hyoid bone to thoroughly remove the cyst wall or sinus tract, with dissection extending upward to the base of the tongue. Ligation of the duct is necessary to prevent recurrence. Intraoperative frozen section analysis is performed to rule out malignant transformation.