Craniostenosis, also known as craniosynostosis or premature cranial suture ossification, is characterized by the premature closure of one or more cranial sutures. This leads to a smaller and abnormally shaped cranial cavity that cannot accommodate the developing brain. Compression and restriction of the rapidly growing brain result in increased intracranial pressure and various neurological dysfunctions.
Clinical Manifestations
Cranial Deformities
Cranial deformities vary depending on the affected suture(s). Premature closure of the sagittal suture results in scaphocephaly or dolichocephaly (elongated skull). Bilateral premature closure of the coronal sutures leads to brachycephaly or flat head deformity. Unilateral premature closure of the coronal suture results in plagiocephaly (asymmetric skull). Premature closure of the metopic suture leads to trigonocephaly (triangular-shaped forehead). When all cranial sutures close prematurely, oxycephaly or tower skull deformity develops, which should be differentiated from microcephaly. Microcephaly is secondary to poor brain development and is not associated with craniosynostosis or increased intracranial pressure.
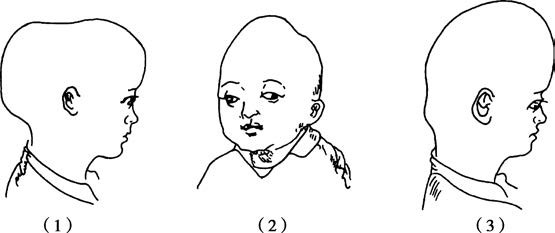
Figure 1 Types of craniostenosis
1, Scaphocephaly
2, Oxycephaly
3, Brachycephaly
Neurological Dysfunction and Increased Intracranial Pressure
Some affected children may present with intellectual disabilities, lethargy, or increased irritability. Vision impairments are common, and late-stage cases may progress to optic atrophy, visual field deficits, or complete blindness. Signs of increased intracranial pressure are often atypical.
Ocular Symptoms and Associated Malformations
Associated findings may include shallow and narrow orbits, proptosis, abnormal orbital spacing, and strabismus. Additional malformations are frequently seen in other parts of the body, such as syndactyly, cleft palate, cleft lip, or spina bifida.
Diagnosis
Diagnosis is generally straightforward based on the characteristic cranial features described above. Plain X-rays of the skull reveal premature disappearance of cranial sutures, replaced by areas of increased bone density at the fusion sites. Additional findings include increased impressions of cerebral gyri and thinning of the sella turcica, indicating raised intracranial pressure. Three-dimensional CT imaging provides a comprehensive view of cranial morphology from multiple angles.
Treatment
Early surgical intervention yields better outcomes, with the prognosis being more favorable for children operated on within the first 6 months of life. Neurological symptoms such as optic atrophy or intellectual disability are usually irreversible even after surgery. The surgical approach varies depending on the affected suture(s) and age of the child. The general principle of surgery involves removing the ossified suture, expanding the cranial cavity, and addressing both cosmetic and neurological developmental needs.