Congenital hydrocephalus, also known as infantile hydrocephalus, refers to a pathological condition that occurs during the embryonic or infantile period. It arises from an imbalance between cerebrospinal fluid (CSF) production and absorption, disruptions in CSF circulation, and/or abnormalities in brain development. This condition leads to excessive CSF within the ventricular system or abnormal brain parenchymal development, resulting in ventricular enlargement. Since the cranial sutures have not yet closed, compensatory cranial expansion occurs, causing characteristic cranial and ocular signs and leading to impaired brain functionality. The incidence of congenital hydrocephalus ranges from 2‰ to 5‰.
Classification
Obstructive Hydrocephalus
This type is caused by obstructions within the ventricular system, such as tumors. The obstruction often occurs in narrow parts of the ventricular system, such as the interventricular foramen, cerebral aqueduct, or the exits of the fourth ventricle. The portions of the ventricular system proximal to the obstruction may significantly enlarge.
Communicating Hydrocephalus
This type results from obstructions in the CSF pathway beyond the fourth ventricle exits or from impaired absorption of CSF.
Additionally, hydrocephalus can be categorized based on its progression rate as acute, chronic, or arrested hydrocephalus; or based on intracranial pressure as high-pressure, normal-pressure, or low-pressure hydrocephalus.
Etiology
The exact cause of congenital hydrocephalus remains unclear. Some cases are associated with mutations in multiple pathogenic genes, while others are more commonly attributed to factors such as tumors, hemorrhage, infections, and trauma. When this condition occurs during the embryonic or infantile periods, it has a particularly severe impact on brain development.
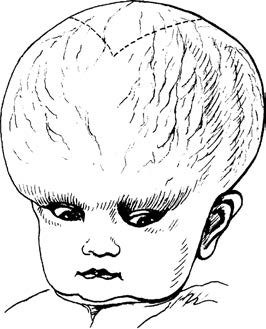
Figure 1 The appearance of congenital hydrocephalus.
The dashed line indicates an enlarged anterior fontanelle.
Excessive CSF Production
Excessive CSF secretion may result from infections, hemorrhages, inflammation, or choroid plexus tumors.
Impaired CSF Absorption
Impediments to CSF absorption may result from infection, hemorrhage, or inflammation causing adhesions in the subarachnoid space. Other significant causes include dural sinus thrombosis and superior vena cava obstruction syndrome.
Obstruction in CSF Circulation
Obstruction within the CSF circulation pathway may arise from conditions such as cerebral aqueduct stenosis, intraventricular tumors, or blood clots. Furthermore, genetic mutations may lead to cilia dysfunction, resulting in abnormal CSF dynamics.
Clinical Manifestations
The clinical presentations of hydrocephalus vary widely across different age groups. In newborns and infants, clinical symptoms differ from those in adults due to incomplete development and limited ability to express symptoms, requiring careful examination.
Symptoms Caused by Increased Intracranial Pressure
During the progressive stages of hydrocephalus, patients with closed cranial sutures typically exhibit the triad of headache, vomiting, and papilledema. In contrast, infants often present with feeding difficulties, irritability, and lethargy.
Abnormal Head Circumference and Head Shape
A head circumference that increases by more than 2 cm per month in infants, especially when accompanied by an enlarged anterior fontanelle and widened cranial sutures, warrants close attention. Other indicators suggesting hydrocephalus include thin scalp, prominent scalp veins, the "setting sun" sign, and macrocephaly.
Neurological Dysfunction
Optic pathway involvement may lead to acute or chronic vision decline. Abducens nerve paralysis can cause strabismus, while oculomotor nerve damage may result in diplopia. Enlargement of the lateral ventricles may stretch or compress the corona radiata, causing gait disturbances and impaired bowel control. Further increases in intracranial pressure may lead to worsening levels of consciousness, progressing from drowsiness to coma. In cases where high intracranial pressure stabilizes and becomes compensated, symptoms may present as ventricular enlargement and cortical atrophy. Affected children often exhibit significant delays in neurodevelopment; however, head circumference ceases to increase, and clinical symptoms stop worsening, indicating arrested hydrocephalus.
Hydrocephalus Caused by Germline Genetic Mutations
These cases often present with multisystem syndromes as part of the clinical picture.
Auxiliary Examinations
Lumbar Puncture
Lumbar puncture can be used to measure intracranial pressure, obtain samples for laboratory analysis, and inject radionuclides or contrast agents for cisternography to determine the location of obstruction. However, there is a risk of causing brain herniation.
Head CT
CT is a safe and rapid method that can reveal the location and degree of ventricular enlargement while identifying potential causes. The Evan’s index, calculated as the ratio between the widest diameter of the frontal horn and the maximum inner diameter of the skull at the same level, is utilized to evaluate the extent of ventricular enlargement.
Head MRI
MRI is generally more sensitive than CT and provides accurate imaging of the shape, size, and narrowed areas of the ventricles and subarachnoid spaces. CSF cine imaging can assess cerebrospinal fluid circulation dynamics.
Head Ultrasound
Ultrasound can monitor and assess ventricular morphology and, in some cases, identify causes such as intraventricular or extraventricular hemorrhage.
Genetic Testing
Testing for mutations in germline pathogenic genes, such as TRIM71 and SMARCC1, can contribute to identifying the underlying cause.
Treatment
Approximately 20% of affected infants exhibit symptom relief and cessation of disease progression through diuretic or dehydration treatment or even without intervention. However, most cases require treatment. The commonly employed approaches are as follows:
Non-Surgical Treatment
Medication-based treatment includes the use of acetazolamide and dehydration agents. These treatments may be effective in cases involving dural venous sinus obstruction or neonatal intraventricular hemorrhage. Repeated lumbar punctures can alleviate hydrocephalus caused by the latter in some cases.
Surgical Treatment
Currently, surgical options include ventriculoperitoneal shunting and endoscopic third ventriculostomy.
Ventriculoperitoneal Shunting
This is the most commonly applied procedure. A burr hole is created in the skull, and the ventricular end of the shunting tube is inserted into the ventricle. The system is connected to a control valve, and the distal catheter is tunneled subcutaneously into the abdominal cavity.
Endoscopic Third Ventriculostomy
A neuroendoscope is used to create an opening in the anterior portion of the floor of the third ventricle, establishing communication between the third ventricle and the basal cisterns. This technique is primarily applied in cases of obstructive hydrocephalus.