Orbital lymphoma is the most common primary malignant orbital tumor in adults. It occurs more frequently in males and predominantly affects middle-aged and elderly individuals. It is typically unilateral and most commonly classified as extranodal marginal zone B-cell lymphoma of mucosa-associated lymphoid tissue (MALT), which is characterized by low malignancy.
Clinical Manifestations
Orbital lymphoma can arise in different orbital quadrants, with the superolateral quadrant being the most commonly involved. Clinical signs primarily include proptosis and eyelid swelling. Additional symptoms may include pain, conjunctival edema, restricted eye movement, diplopia, and vision loss. CT imaging often reveals a tumor with unclear margins, which may encase the extraocular muscles.
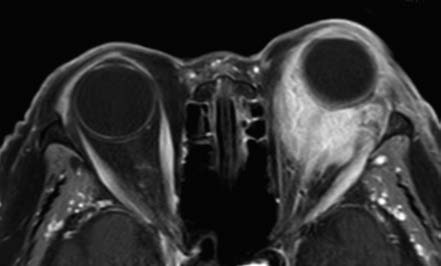
Figure 1 Imaging features of left orbital lymphoma
Contrast-enhanced axial T1-weighted MRI shows the tumor encasing the eyeball with a mold-like appearance and significant enhancement.
MRI typically demonstrates intermediate signal intensity on T1-weighted imaging (T1WI) and high signal intensity on T2-weighted imaging (T2WI), with marked enhancement on contrast imaging. When the tumor encases the eyeball, it may present with a mold-like appearance. Orbital lymphoma can be challenging to differentiate from benign conditions such as nonspecific orbital inflammatory disease; biopsy is often required for definitive diagnosis.
Treatment
Orbital lymphoma is highly radiosensitive, and radiotherapy is the primary treatment modality. Surgical resection is mainly performed for superficial focal lesions. Chemotherapy is indicated for patients with systemic lymphoma. The addition of targeted therapies to conventional chemotherapy regimens may improve treatment outcomes.