Vitreoretinal lymphoma is considered part of central nervous system lymphoma, with most cases classified as diffuse large B-cell lymphoma. A smaller proportion is associated with T-cell and natural killer T-cell lymphoma. It predominantly occurs in middle-aged and elderly individuals, with the incidence rate in females being 1.3 to 2 times higher than in males.
Clinical Manifestations
Clinical symptoms include visual impairment, blurred vision, and/or floaters. The condition can be categorized into three clinical types based on signs:
- Vitreous Type: Involves only vitreous tumor cells without retinal infiltration.
- Retinal Type: Involves retinal lesions exclusively.
- Vitreoretinal Type: Includes features of both types above.
Ocular manifestations can be summarized as follows:
- Various types of keratic precipitates (KP).
- Rare findings such as iris depigmentation, scleritis, or pseudo-hyphema.
- Variable degrees of vitreous cellular infiltration, with cells often appearing in sheet-like or cluster arrangements.
- Multifocal, cream-colored retinal lesions in the outer layers of the retina, often accompanied by leopard-like fundus patterns, atrophy or fibrosis of the retinal pigment epithelium (RPE).
- Additional findings such as retinal hemorrhage, retinal vasculitis, macular edema, retinal detachment, and necrotizing retinitis.
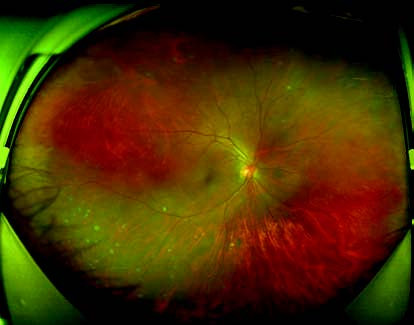
Figure 1 Wide-angle fundus photograph of the right eye in vitreoretinal lymphoma
Multifocal, cream-colored retinal lesions with poorly defined borders are visible, accompanied by a leopard-spot appearance of the fundus.
Due to its complex and diverse clinical presentations, the condition is frequently misdiagnosed as uveitis.
Diagnosis
Vitreous cell biopsy remains the "gold standard" for diagnosing primary vitreoretinal lymphoma. An intraocular cytokine IL-10/IL-6 ratio greater than 1, along with positive detection of MyD88 gene mutations, serves as important diagnostic indicators. Additional diagnostic tools include IgH and TCR gene rearrangement, flow cytometry, and immunohistochemistry. Combining these tests with specialized imaging techniques such as ocular OCT, FFA, ICGA, and fundus autofluorescence can improve diagnostic accuracy.
Treatment
Therapy is divided into ocular and systemic treatments. Intravitreal methotrexate injection is the primary method for local treatment and is effective in controlling intraocular lesions, although it does not prevent central nervous system dissemination. Systemic treatments aim to reduce CNS involvement and include intravenous chemotherapy, intrathecal chemotherapy, cranial irradiation, and peripheral blood stem cell transplantation.