Melanoma of the lacrimal sac, a subtype of mucosal melanoma, ranks as the second most common non-epithelial malignant tumor of the lacrimal sac. The condition is prone to recurrence and metastasis, leading to a poor prognosis.
Clinical Presentation
The disease is more prevalent in middle-aged and elderly individuals, with no significant gender difference. In the early stages, common symptoms include epiphora and mucopurulent discharge, which are often misdiagnosed as chronic dacryocystitis. As the condition progresses, symptoms such as bloody tears, pain, epistaxis, proptosis, or systemic manifestations may develop. A firm, poorly tender mass in the medial canthal region typically becomes palpable in most patients about six months after the onset of epiphora. The tumor exhibits highly invasive behavior, with a tendency to infiltrate the paranasal sinuses and orbit and to metastasize systemically. CT imaging reveals an irregular mass in the lacrimal sac region with destruction of the medial orbital wall and the bony structure of the nasolacrimal duct, accompanied by invasion into the ethmoid sinus or nasal cavity. MRI findings show the tumor as exhibiting intermediate to high signals on T1-weighted images and intermediate to low signals on T2-weighted images, with inhomogeneous enhancement after contrast administration. Pathological examination commonly identifies epithelioid cell types, characterized by eosinophilic cytoplasm, round nuclei with prominent nucleoli, and the presence of melanin granules in the cytoplasm.
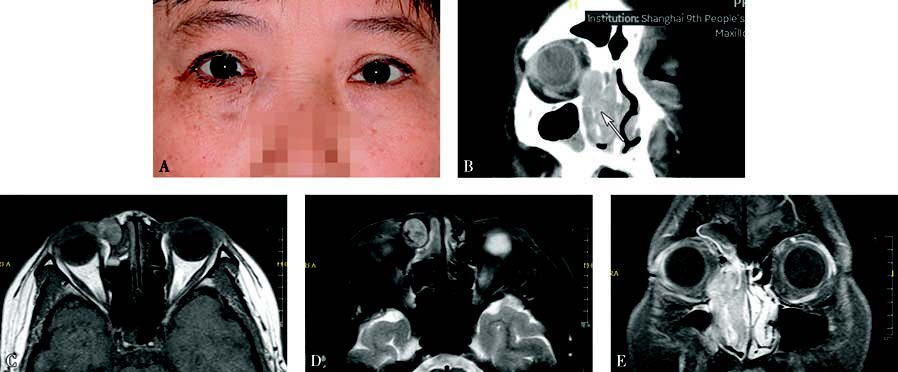
Figure 1 Appearance and imaging of a patient with right lacrimal sac melanoma
A. The patient presents with epiphora and bloody tears in the right eye. A black mass is visible at the lower lacrimal punctum, elevated above the lid margin, with a bulge in the medial canthal region.
B. Coronal CT shows an irregular mass in the lacrimal sac region, with destruction of the medial orbital wall and the nasolacrimal duct's bony structures, along with invasion into the ethmoid sinus and nasal cavity (white arrow).
C. Axial T1-weighted MRI demonstrates the tumor with intermediate to high signals.
D. Axial T2-weighted MRI shows the tumor with intermediate to low signals.
E. Coronal contrast-enhanced T1-weighted MRI reveals inhomogeneous enhancement of the mass.
Treatment
Radical excision surgery is the primary treatment, with biopsy generally avoided unless necessary. Postoperative therapy usually involves a combination of radiotherapy, chemotherapy, and targeted therapies.