A complex orbital fracture refers to fractures involving the orbital rim and the adjacent bones, including the zygomatic bone, maxilla, nasal bone, lacrimal bone, and frontal bone. These fractures are typically classified based on their extent and location and are divided into zygomaticomaxillary fractures, nasoorbitoethmoidal fractures, frontoorbital fractures, and multiple orbital fractures.
Clinical Manifestations
Symptoms and signs vary widely due to differences in the location, range, and severity of the fractures. In addition to common features seen in orbital fractures, such as enophthalmos, ocular motility restriction, and diplopia, complex orbital fractures exhibit specific manifestations:
Zygomaticomaxillary Fracture
Often presents with flattening of the lateral orbital region, downward and outward displacement of the orbit, abnormal facial protrusion, and numbness in areas innervated by the infraorbital nerve. If the fracture involves the temporomandibular joint, varying degrees of impairment in masticatory function may occur.
Nasoorbitoethmoidal Fracture
Characteristic features include rounding and displacement of the medial canthal area, an increased intercanthal distance, protrusion or depression at the medial orbital rim, and localized deformities. Damage to the nasolacrimal duct may lead to epiphora or purulent discharge.
Frontoorbital Fracture
Involvement of the orbital roof, supraorbital rim, frontal bone, or frontal sinus is common and is often associated with traumatic brain injuries. Symptoms may include numbness in the area innervated by the supraorbital nerve, deformities or depressions in the supraorbital region, ptosis, and other abnormalities.
CT imaging is the standard diagnostic tool for complex orbital fractures. Three-dimensional reconstruction based on imaging data allows clear visualization of the location, extent, and severity of the fractures.
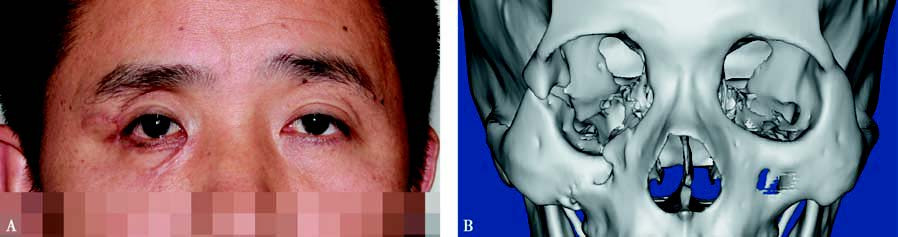
Figure 1 Right zygomaticomaxillary fracture
A: Patient’s facial appearance. B: CT 3D reconstruction of the orbit.
Treatment
Surgical intervention is the primary treatment for complex orbital fractures, with the general approach focusing on the simultaneous repair of orbital rim fractures and orbital wall defects.
For patients with severe fractures where anatomical landmarks are lost, endoscopic navigation technology is recommended to assist in guiding reconstruction surgeries.
Patients with zygomaticomaxillary fractures that do not cause significant displacement of the zygomatic body or functional impairments may not require surgical treatment. However, if the zygomatic body is displaced, resulting in deformities such as collapse, restricted ocular movement, diplopia, or limited mouth opening, surgery is necessary. Surgical treatment of nasoorbitoethmoidal fractures typically involves reconstructing the orbit, correcting medial canthal deformities, and repairing damaged nasolacrimal ducts.
In cases of frontoorbital fractures, surgical priorities include restoring the anatomical position of the frontal bone, correcting orbital roof depressions, removing bone fragments, and improving ocular motility.