Crouzon syndrome is a craniofacial disorder resulting from the premature fusion of cranial sutures, such as the coronal, sagittal, or lambdoid sutures. This premature fusion leads to various craniofacial developmental abnormalities. The syndrome is characterized by cranial deformities (scaphocephaly or trigonocephaly), facial anomalies (a beak-shaped nose and mandibular prognathism), bilateral exophthalmos, and strabismus. The estimated prevalence is approximately 1 in 25,000 live births.
Clinical Manifestations
Crouzon syndrome primarily presents with typical features affecting the skull, eyes, and oral and maxillofacial region:
Cranial Suture Synostosis
The most commonly involved suture is the coronal suture, though sagittal and lambdoid sutures can also be affected. This results in cranial deformities such as brachycephaly, scaphocephaly, or trigonocephaly and is often accompanied by intracranial hypertension.
Ocular Abnormalities
Insufficient anterior-posterior growth of the temporal cranial base leads to inadequate orbital development. Additionally, increased intracranial pressure causes a depressed anterior cranial base and a forward-displaced middle cranial base, resulting in shallow orbits and exophthalmos. In severe cases, eye dislocation may occur. Patients often have bilateral exotropia. Chronic intracranial hypertension can lead to optic nerve and visual pathway damage, resulting in visual impairment.
Oral and Maxillofacial Abnormalities
Patients frequently present with malar hypoplasia, maxillary hypoplasia, and mandibular prognathism. Common dental features include overcrowding of the maxillary dental arch, a V-shaped dental arch, a narrow and highly arched palate, as well as cleft palate and bifid uvula.
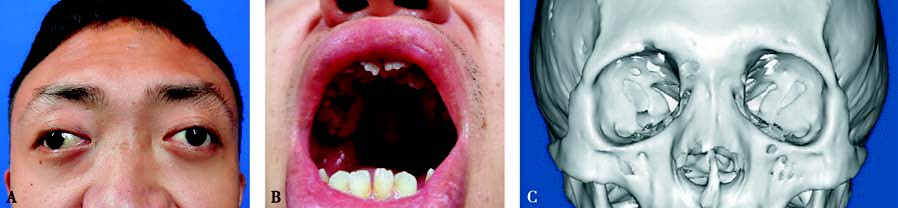
Figure 1 Crouzon syndrome
A. External appearance of the patient showing an acrocephalic skull, bilateral exophthalmos, and exotropia.
B. Intraoral photograph showing crowding of the maxillary teeth, a V-shaped dental arch, and a narrow, highly arched palate.
C. 3D CT reconstruction revealing shallow orbits and underdevelopment of the orbits and maxillary bone.
Treatment
Cranial vault remodeling and/or fronto-orbital reshaping surgery are recommended at 6–12 months of age. For patients with significantly elevated intracranial pressure, early cranial expansion surgery is advised. In adult patients, computer-aided techniques can be utilized to develop distraction osteogenesis plans to guide surgical procedures.