Nystagmus is an involuntary, rhythmic oscillation of the eyes, involving a disturbance in the coordinated function of interactions between neural pathways. It arises from abnormalities in visual, neurological, or vestibular functions, leading to abnormal eye movements.
Classification
Classification by Rhythm
Nystagmus is classified into jerk nystagmus and pendular nystagmus.
Classification by Type
Nystagmus is categorized as horizontal nystagmus, vertical nystagmus, rotary nystagmus, or mixed nystagmus.
Classification by Onset
Nystagmus is divided into congenital nystagmus and acquired nystagmus.
Congenital Nystagmus
Congenital Motor Nystagmus
The exact cause is unknown but is related to genetics, primarily involving efferent mechanism defects. It may affect the central nervous system or conjugate motor pathways, while no abnormalities are present in the eyes. This nystagmus is binocular and conjugate, predominantly horizontal, and remains horizontal during upward or downward gaze. It may present as pendular, jerk, rotary, or a combination of types in the same individual. The waveform in congenital motor jerk nystagmus typically exhibits an exponentially increasing velocity during the slow phase. The intensity of nystagmus often reduces with convergence, frequently associated with esotropia. A null position, where the nystagmus decreases and visual acuity improves, may exist. If this null position is not in the primary gaze, a compensatory head posture may occur to achieve optimal visual acuity at this position.
Sensory Defect Nystagmus
Arises secondary to defects in the visual input pathway. Blurred images at the macula lead to feedback disruption, impairing fixation reflex development, and causing loss of the fine-motion system required to keep targets centered on the fovea. Nystagmus typically appears around 3 months of age in cases of congenital vision loss, with severity depending on the degree of visual impairment. Sensory defect nystagmus is usually pendular in nature but transitions to jerk nystagmus during lateral gaze.
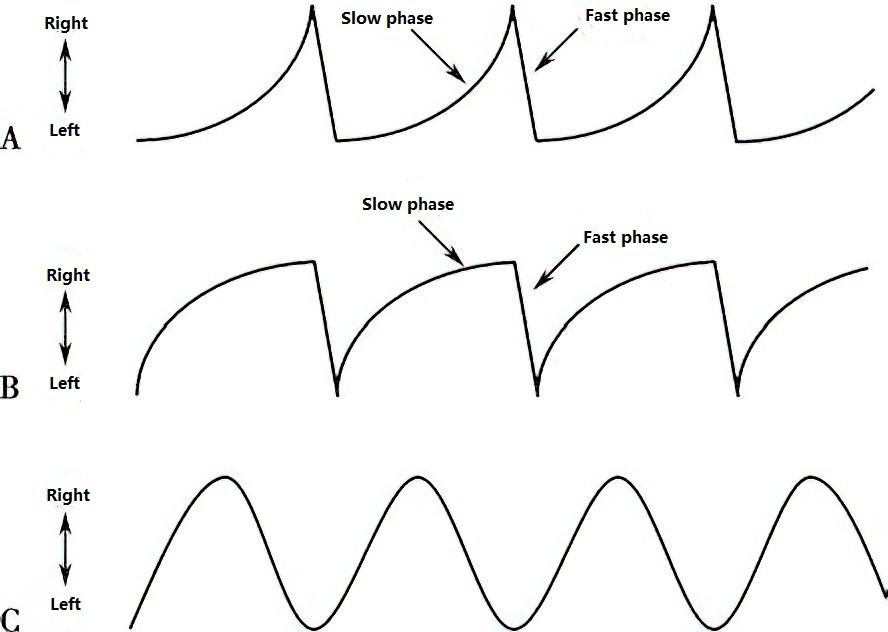
Figure 1 Common eye movement waveforms in congenital nystagmus
A. Jerk nystagmus with exponentially increasing velocity, where the slow-phase eye movement velocity increases exponentially.
B. Jerk nystagmus with exponentially decreasing velocity, where the slow-phase eye movement velocity decreases exponentially.
C. Pendular nystagmus.
Latent Nystagmus
The cause remains unknown. This horizontal jerk nystagmus manifests when one eye is covered, with the fast phase directed toward the uncovered (fixating) eye. It is absent when both eyes are fixating the target binocularly. In cases of manifest-latent nystagmus, the nystagmus amplitude increases, and visual acuity decreases when either eye is covered. The waveform of latent nystagmus is characterized by an exponentially decreasing velocity during the slow phase.
Periodic Alternating Nystagmus (PAN)
The exact cause of PAN is unclear. The direction of nystagmus alternates periodically, with each directional phase lasting approximately 1–1.5 minutes. The amplitude of nystagmus gradually diminishes until it nearly disappears, after which it reverses direction following a brief pause of 10–20 seconds. This cycle continues repetitively. Due to the alteration in nystagmus direction, compensatory head positions may also exhibit alternating changes.
Treatment
There are currently no direct and effective treatments for nystagmus. Available interventions primarily aim to alleviate clinical symptoms.
Refractive Correction
Refractive errors, if present, can be corrected after refractive testing under ciliary muscle paralysis.
Prism Lenses
Prism lenses take advantage of certain features of congenital motor nystagmus, such as a reduction or suppression of nystagmus in the null position or during convergence. They are used to eliminate compensatory head postures and improve visual acuity.
Yoked Prisms
Prism lenses are placed in the same direction for both eyes, with the base opposite to the null position and the apex pointing toward the null position (healthy side). This shifts the null zone from the lateral gaze to the primary gaze, eliminating compensatory head postures.
Base-Out Prisms
Both eyes are fitted with base-out prisms to induce convergence, thereby suppressing nystagmus.
Surgical Treatment
In cases of congenital nystagmus with a null position and compensatory head posture, surgery can reposition the null position from the lateral to the central gaze, reducing or eliminating compensatory head posture and improving visual acuity. However, surgical intervention cannot cure the nystagmus. Pre-surgical prism testing is necessary. If yoked prisms with the apex directed toward the healthy side eliminate or significantly reduce the compensatory head posture, this indicates that the head posture can be corrected surgically.