Dissociated vertical deviation (DVD) is a condition with an unclear pathogenesis, characterized primarily by alternating hypertropia in both eyes. The eye movements do not adhere to Hering’s law of equal innervation, and the eyes exhibit dissociated movements.
Diagnosis
During alternate cover testing, the covered eye drifts upward with associated extorsion, and after uncovering, the eye slowly returns to the primary position with associated intorsion. The condition is more easily revealed during distance fixation. When the head is turned laterally, the presence of alternating upward drift during alternate cover testing distinguishes DVD from isolated inferior oblique overaction. Bielschowsky’s test is performed using a series of filters with varying densities. If the covered eye drifts further upward as the filter density increases, and the hypertropic eye drops beyond the fixation position to a lower position as the filter density decreases, the test is considered positive for Bielschowsky’s sign. DVD may be associated with congenital esotropia, nystagmus, amblyopia, and inferior oblique overaction.
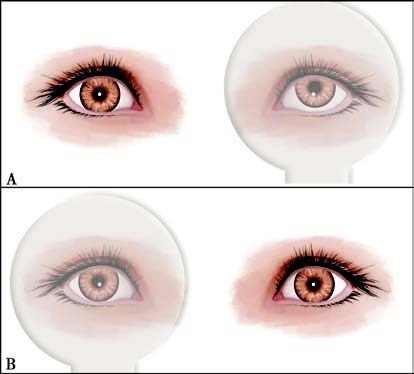
Figure 1 Dissociated vertical deviation
A. Covering the left eye causes significant upward drift of the left eye.
B. Covering the right eye causes mild upward drift of the right eye.
DVD often occurs in both eyes. It can be symmetrical but more commonly presents asymmetrically.
Treatment
If there is no obvious alternating hypertropia under normal conditions and it is only revealed during examination, conservative management is typically employed. In cases associated with refractive errors, optical methods can be used to switch the fixation eye and avoid visible upward drifting. For cases without inferior oblique overaction, treatment is generally focused on weakening the superior rectus muscle. In patients with significant upward drifting, superior rectus recession greater than 7 mm is recommended; alternatively, superior rectus recession combined with posterior fixation suture (Faden procedure) may be performed. For cases involving inferior oblique overaction, an inferior oblique transposition procedure is performed, wherein the distal end of the inferior oblique muscle is fixed to the temporal side of the inferior rectus insertion.