Anisometropia refers to a condition where the refractive error of the two eyes differs in degree or type. However, it is generally recognized that perfectly identical refractive states in both eyes are rare, and mild interocular differences are very common and considered physiological anisometropia. When the spherical refractive difference between the two eyes equals or exceeds 1.50 diopters (D), or the cylindrical difference equals or exceeds 1.00D, various visual problems may arise.
Etiology and Pathogenesis
The development of anisometropia can be attributed to several factors, primarily involving the asymmetrical growth of the two eyes. During childhood development, the difference in axial elongation between the two eyes is the main cause of anisometropia. Other contributing factors include imbalanced axial development, unequal reduction of hyperopia, differing progression rates of myopia, ocular trauma, surgery, or congenital ocular diseases.
Anisometropia is a common cause of amblyopia. Anisometropic amblyopia occurs during the critical period of visual development when untreated abnormal refractive states result in differences in image clarity or size between the two retinas. The brain has difficulty fusing the images and subsequently suppresses the blurred image, leading to persistent visual impairment in the affected eye and eventual amblyopia. Both the type and degree of anisometropia can influence the severity of amblyopia.
As binocular accommodation generally occurs symmetrically (Hering’s law), individuals with anisometropia often experience one eye focusing clearly while the other remains blurred in the uncorrected state. For hyperopic anisometropia, the lower hyperopic or emmetropic eye achieves clear focus, whereas the higher hyperopic eye remains unfocused and is prone to developing amblyopia. Myopic anisometropia tends to result in the lower myopic or emmetropic eye focusing on distant targets, whereas the higher myopic eye is utilized for near vision. This rarely leads to amblyopia but can disrupt binocular visual function due to reduced fusion opportunities.
Classification
Simple Anisometropia
Simple Myopic Anisometropia
One eye is emmetropic, while the other is myopic.
Simple Hyperopic Anisometropia
One eye is emmetropic, while the other is hyperopic.
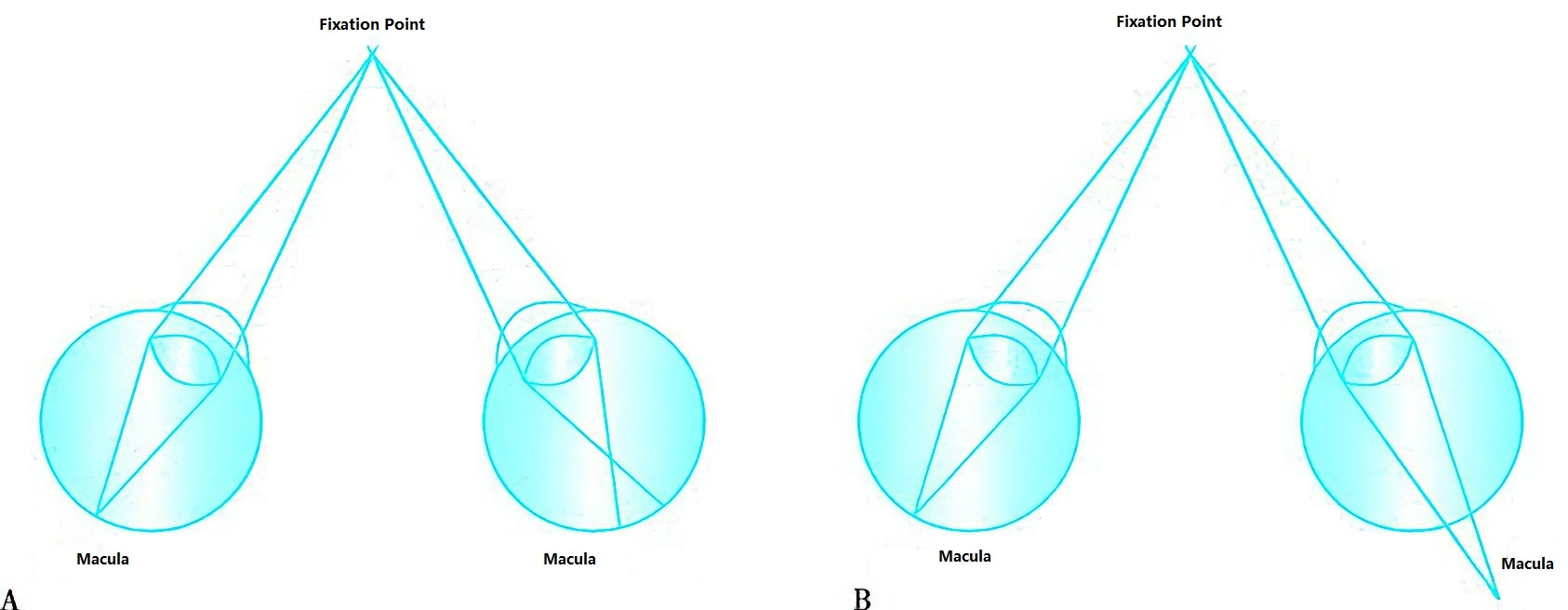
Figure 1 Anisometropia
A. Myopic Anisometropia
B. Hyperopic Anisometropia
Compound Anisometropia
Compound Myopic Anisometropia
Both eyes are myopic, but to different degrees.
Compound Hyperopic Anisometropia
Both eyes are hyperopic, but to different degrees.
Mixed Anisometropia
One eye is hyperopic, and the other is myopic.
Simple Astigmatic Anisometropia
One eye is emmetropic, while the other has either myopic, hyperopic, or mixed astigmatism.
Compound Astigmatic Anisometropia
Both eyes have astigmatism, but the type or degree differs between the eyes.
Other Forms of Anisometropia
Relative Anisometropia
In this type, both eyes share the same refractive state, but a significant difference in axial length results in unequal retinal image sizes. This is a special type of anisometropia caused by differences in axial length.
Diagnosis
Patients with anisometropia may present with symptoms such as visual fatigue, binocular single vision dysfunction, or alternating eye use. Diagnosis typically involves cycloplegic refraction to obtain the exact refractive power of both eyes. Anisometropia is confirmed when the spherical refractive difference between the eyes equals or exceeds 1.50 diopters, or the cylindrical difference equals or exceeds 1.00 diopters.
Management
The primary goal of anisometropia correction is to ensure that both eyes achieve adequate or nearly adequate correction for optimal visual acuity, balanced binocular vision, and similar retinal image sizes. Current treatment options include correction using eyeglasses, contact lenses, or surgical methods.
In cases where anisometropic refractive error is fully corrected, differences in the size of retinal images may arise, a condition known as aniseikonia, which can cause difficulties with fusion. This may manifest as symptoms such as dizziness or blurred vision during reading. Due to the magnification effect of spectacle lenses, patients with anisometropia greater than 2.50 diopters often experience fusion-related symptoms when corrected with eyeglasses. Contact lenses provide a more effective correction for patients with significant anisometropia.
Since contact lenses rest on the cornea, the retinal image size they produce is closer to that of an emmetropic eye. Additionally, unlike eyeglasses, contact lenses avoid prismatic effects during eye movements and, through a tear film lens effect, provide better correction for corneal astigmatism, yielding clearer image quality. For instance, in cases where one eye is aphakic, wearing eyeglasses may result in about a 25% difference in retinal image size, making fusion extremely difficult. In contrast, contact lenses reduce the size difference to approximately 6%, which is within the fusion capacity of the eyes (approximately 5%), thus alleviating fusion-related visual symptoms. Therefore, the magnification effects of different corrective methods must be considered when managing anisometropia.
Due to the relationship between anisometropia and aniseikonia, binocular visual function is often impaired. Clinical studies show that individuals with mild anisometropia can maintain normal binocular function, but as the degree of anisometropia increases, the likelihood of abnormal stereopsis rises. When anisometropia exceeds 3.00 diopters, the prevalence of abnormal stereopsis approaches 100%. Consequently, when managing anisometropia, assessing binocular visual function is an important consideration.