This condition is typically caused by damage from tumors in adjacent tissues (primarily pituitary adenomas and craniopharyngiomas), vascular lesions (such as internal carotid artery aneurysms or posterior communicating artery aneurysms), or demyelinating diseases. It is characterized by homonymous hemianopia on the side opposite to the lesion in both eyes. For example, a lesion in the left optic tract results in visual field defects involving the nasal field of the left eye and the temporal field of the right eye. Because the crossed and uncrossed optic nerve fibers in the optic tract are not arranged symmetrically on both sides, the visual field defects in the two eyes may not be consistent.
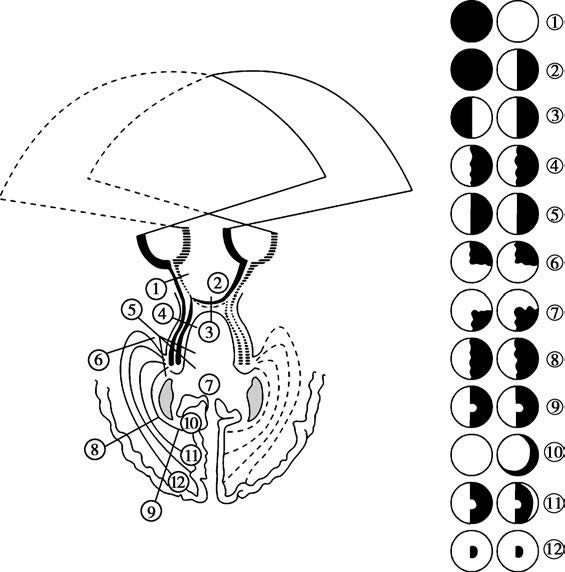
Figure 1 Schematic representation of visual field defects caused by lesions at different locations of the visual pathway.
Solid lines represent the retinal regions of the temporal side of the left eye and the nasal side of the right eye; uncrossed temporal optic nerve fibers of the left eye; crossed nasal optic nerve fibers of the right eye; the left optic tract; the left optic radiation.
Dashed lines represent the retinal regions of the temporal side of the right eye and the nasal side of the left eye; uncrossed temporal optic nerve fibers of the right eye; crossed nasal optic nerve fibers of the left eye; the right optic tract; the right optic radiation.
1, Optic nerve → Complete blindness in the affected eye.
2, Junction of the optic nerve and chiasm → Blindness in the affected eye and temporal hemianopia in the contralateral eye.
3, Central part of the optic chiasm → Bitemporal hemianopia.
4, Optic tract → Asymmetric homonymous hemianopia.
5, Posterior part of the optic tract, lateral geniculate body, or inferior part of the optic radiation → Prominent homonymous hemianopia without macular sparing.
6, Anterior loop of the optic radiation → Asymmetric superior quadrantanopia.
7, Interior part of the optic radiation → Mildly asymmetric inferior quadrantanopia.
8, Middle part of the optic radiation → Mildly asymmetric homonymous hemianopia.
9, Posterior part of the optic radiation → Symmetric homonymous hemianopia with macular sparing.
10, Anterior part of the calcarine fissure → Crescent-shaped defects in the contralateral eye's visual field.
11, Middle part of the calcarine fissure → Symmetric homonymous hemianopia with macular sparing and crescent-shaped temporal field sparing in the contralateral eye.
12, Occipital pole → Symmetric homonymous central scotoma.
Since pupillary nerve fibers accompany the optic tract, optic tract lesions may result in Wernicke’s hemianopic pupillary reaction, where shining light on the retina on the hemianopic side does not cause pupillary constriction. In the late stages of the condition, descending optic nerve atrophy may occur.
Treatment
Treatment is directed at addressing the underlying disease.