Coats disease is a condition with an unclear etiology. It commonly occurs in healthy male children, with most cases appearing before the age of 10, typically affecting only one eye. However, cases in other age groups and adults are not uncommon.
Clinical Manifestations
Infants and young children are often brought to medical attention when parents notice strabismus or leukocoria (a white pupil) in the affected eye. School-aged children are frequently diagnosed during vision screening when reduced vision in one eye is detected. At the time of diagnosis, fundus changes are often in the advanced stages. In the early stages, lesions are usually located temporally, most commonly in the area beyond the second branch of the retinal blood vessels. Affected vessels show pronounced tortuosity and irregular saccular or beaded dilations, with dot or patchy hemorrhages in the retina. Neovascularization is relatively rare. In the deeper layers of the retina and the subretinal space within the affected region, yellow-white lipid exudates are deposited in sheets or distributed in a ring around the abnormal vessels. Shiny cholesterol crystals can occasionally be observed. In cases involving the macula, hard exudates with a stellate or annular pattern may be seen, and subretinal fibrosis in the macular area can develop in the advanced stages. Significant fluid exudation may lead to exudative retinal detachment. Severe cases can result in complications such as iridocyclitis, neovascular glaucoma, secondary cataracts, and eventual phthisis bulbi. Fundus fluorescein angiography (FFA) shows abnormal dilation and tortuosity of small arteries, veins, and capillaries in the affected area, along with microaneurysm formation and patchy capillary nonperfusion. Fluorescein leakage may also be observed.
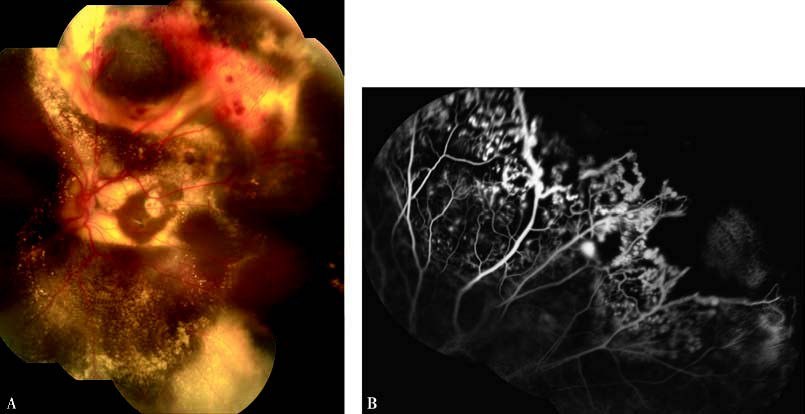
Figure 1 Coats disease in the left eye
Panel A: A color fundus photograph showing subretinal yellow-white lipid exudate deposition with localized retinal detachment. Capillary dilation and microaneurysms are visible in the superotemporal periphery.
Panel B: FFA demonstrating retinal microvascular dilations, terminal aneurysmal expansions in the superotemporal periphery, and regions of capillary nonperfusion in the peripheral retina.
In pediatric patients, the differential diagnosis includes retinoblastoma.
Treatment
Early-stage lesions may be treated with laser photocoagulation or cryotherapy. For cases with exudative retinal detachment, treatment combinations may include intravitreal anti-vascular endothelial growth factor (anti-VEGF) injections, laser photocoagulation or cryotherapy, and scleral drainage procedures. In advanced cases, a combination of treatments such as vitrectomy, retinal reattachment surgery, retinal laser photocoagulation or cryotherapy, and intravitreal anti-VEGF injections are used to preserve part of the affected eye.