The cilioretinal artery typically enters the retina from the temporal side of the optic disc, functioning independently of the central retinal artery (CRA). Fluorescein Fundus Angiography (FFA) has shown that approximately 32% of eyes in the population have a cilioretinal artery. On ophthalmoscopy, cilioretinal artery occlusion appears as regional superficial retinal pallor along the distribution of the cilioretinal artery. Clinically, three variants have been identified:
- Isolated cilioretinal artery occlusion.
- Cilioretinal artery occlusion associated with central retinal vein occlusion (CRVO).
- Cilioretinal artery occlusion associated with anterior ischemic optic neuropathy.
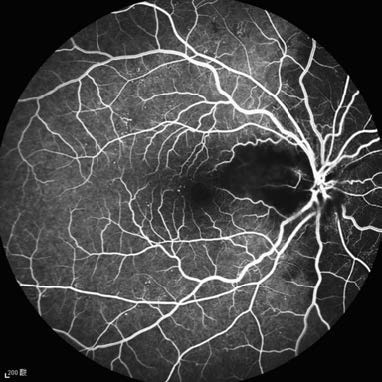
Figure 1 Fluorescein angiography of cilioretinal artery occlusion in the right eye
The area supplied by the cilioretinal artery shows weak blood flow signals, presenting as a filling defect.
The systemic etiological workup for isolated cilioretinal artery occlusion is the same as that for CRAO. Cases associated with CRVO are generally due to localized causes. For cases accompanied by anterior ischemic optic neuropathy, giant cell arteritis should be considered as a potential underlying cause and evaluated accordingly.