Familial exudative vitreoretinopathy (FEVR) is a predominantly autosomal dominant inherited ocular disease.
Clinical Manifestations
Symptoms
Mild cases are often asymptomatic.
Ocular Findings
Fundus examination may reveal early features such as an increased number of retinal vascular branches and vascular straightening in the temporal periphery. Additional findings may include retinal capillary telangiectasia, abnormal peripheral vascular anastomoses, avascular zones, neovascularization, and leakage.
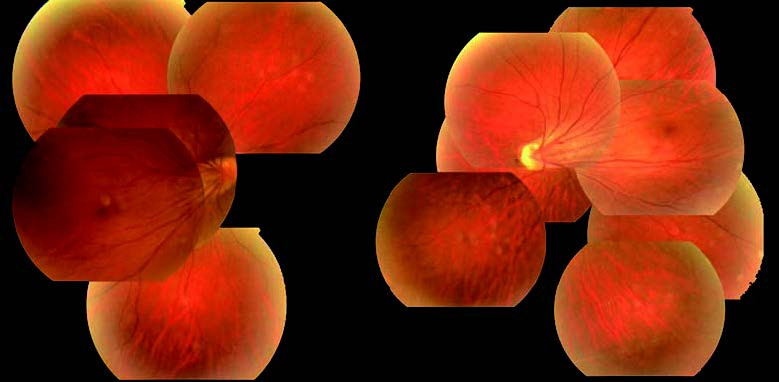
Figure 1 Familial exudative vitreoretinopathy (FEVR)
The image originates from a 40-year-old male patient, whose children all exhibit similar alterations.
As the disease progresses, vitreous and fibrous proliferation can produce traction, leading to macular ectopia, retinal folds, retinal detachment, and posterior lens capsule fibrous proliferation.
In the neonatal or adolescent period, subretinal exudation or exudative retinal detachment may occur.
In advanced stages, anterior segment involvement may develop, and even phthisis bulbi can occur.
FEVR typically presents with asymmetric changes in both eyes. Fundus changes are similar to those seen in retinopathy of prematurity (ROP) but occur in full-term infants, particularly in those with a family history. Family members may show peripheral vascular traction or avascular zones in their fundus.
Differential Diagnosis
Retinopathy of prematurity usually occurs in low-birth-weight preterm infants with a history of significant oxygen exposure. It frequently involves poorly vascularized peripheral retina and begins with proliferative changes in the temporal periphery. In contrast, FEVR often occurs in full-term infants without a history of oxygen exposure.
Treatment
Peripheral retinal avascular zones with any evidence of disease activity may be treated with laser photocoagulation or cryotherapy. Anti-VEGF agents injected into the vitreous cavity may be used to suppress retinal neovascularization. Retinal detachment, if present, requires prompt surgical intervention.