Under normal circumstances, the lens is suspended on the ciliary body by the zonules of Zinn. The anteroposterior axis of the lens is almost aligned with the visual axis. Partial or complete rupture or deficiency of the zonules can weaken the suspensory force, leading to abnormal positioning of the lens. If the lens is not in its normal position at birth, this condition is referred to as ectopia lentis (congenital lens dislocation). If the lens position changes after birth due to congenital factors, trauma, or certain diseases, it is termed lens dislocation.
Etiology
Incomplete development or loosening of the zonules (congenital); rupture of the zonules due to trauma; and certain intraocular conditions can all lead to lens dislocation or subluxation. Intraocular pathologies such as staphyloma, buphthalmos, or globe enlargement may cause mechanical elongation of the zonules. Inflammatory processes within the eye, such as cyclitis, can induce zonular degeneration, resulting in displacement of the lens.
Clinical Features
Traumatic lens dislocation is often associated with a history of ocular contusion and other external signs of injury. Congenital lens dislocation frequently occurs in association with genetic disorders, such as Marfan syndrome, Marchesani syndrome, and homocystinuria.
Complete Lens Dislocation
In cases where all zonules are ruptured, the lens may fully dislocate into the following positions.
Anterior Chamber
The lens usually sinks to the inferior part of the anterior chamber. The diameter of the lens appears smaller than it does in its normal position, while the curvature increases. The lens's edge may exhibit a golden luster, giving a transparent lens an oil-drop appearance. An opaque lens appears white and disc-shaped. The dislocated lens may press against the iris and interfere with the anterior chamber angle, obstructing aqueous humor outflow and causing acute intraocular pressure elevation.
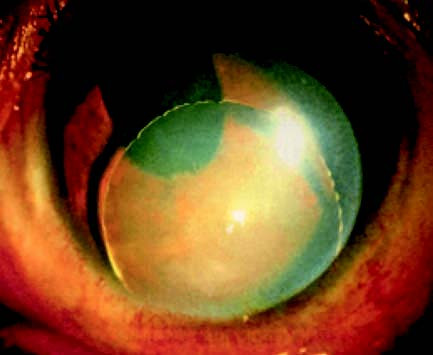
Figure 1 Lens dislocated into the anterior chamber
Vitreous Chamber
The lens appears as a transparent spherical object. In the early stages, it may remain mobile, but over time it becomes fixed in the lower part of the vitreous chamber and may adhere to the retina. Prolonged dislocation can lead to lens opacification, lens-induced uveitis, and secondary glaucoma.
Embedded in the Pupillary Zone
The lens may partially protrude into the anterior chamber, impairing aqueous humor circulation and leading to acute intraocular pressure elevation.
Outside the Globe
Severe trauma can cause limbal rupture, allowing the lens to dislocate beneath the conjunctiva or even completely out of the eye. Once fully dislocated from the pupillary area, vision in the affected eye is akin to aphakia (absence of the lens). The anterior chamber deepens, and iris tremor occurs. In the early stages, the lens may move in response to changes in body position.
Subluxation of the Lens
Subluxation presents with part of the lens visible in the pupillary zone, and the equatorial region of the lens can be observed after pupil dilation. Zonular rupture occurs in the affected area. Symptoms depend on the degree of lens displacement. If the anteroposterior axis remains aligned with the visual axis, lens-induced myopia may occur due to zonular stretching and subsequent increased lens curvature. Subluxation may also result in monocular diplopia, with one image formed via the lens and a smaller, secondary image seen through the aphakic portion of the visual field.
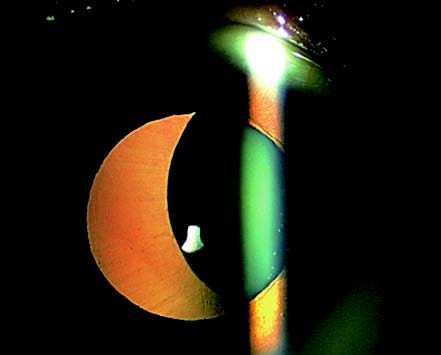
Figure 2 Lens subluxation (Marfan syndrome)
Diagnosis
A definite diagnosis can usually be made based on the patient’s medical history, symptoms, and slit-lamp microscope findings.
Treatment
Non-Surgical Treatment
For subluxated or vitreous-dislocated lenses that remain transparent and have not caused severe complications, close monitoring is an option. Some patients may achieve partial functional vision with correction using convex lenses or contact lenses.
Surgical Treatment
Advances in modern vitreoretinal microsurgical techniques have expanded the indications for surgical intervention in cases of lens dislocation. Surgery becomes necessary for dislocated lenses that have dissolved, become opaque, or caused severe complications. Lenses dislocated into the anterior chamber or embedded in the pupil also require timely surgical treatment.