Bullous keratopathy refers to corneal stromal edema and subepithelial bullae formation resulting from severe damage to corneal endothelial cells. This condition arises due to endothelial cell decompensation, leading to the loss of both the fluid barrier and active fluid pump functions. It can occur as a consequence of anterior segment surgeries, particularly cataract extraction and/or intraocular lens implantation, corneal endothelial dystrophy, endothelial contact with vitreous prolapse in aphakic eyes, chronic elevated intraocular pressure or glaucoma surgeries, and endothelial damage caused by herpes simplex or herpes zoster virus infections.
Clinical Manifestations
Patients often have a history of the aforementioned conditions. Affected individuals experience blurred vision, which tends to be worse in the morning and may improve as the day progresses in milder cases. Severe cases are associated with pronounced irritation symptoms, including pain, tearing, and photophobia, with symptoms peaking when epithelial bullae rupture. Mixed conjunctival hyperemia, corneal stromal edema with thickening, a hazy or bullous epithelial surface, and an unclear or irregularly folded posterior corneal interface are frequently observed. Prolonged disease may result in the formation of corneal stromal neovascularization and stromal haze, causing significant visual decline.
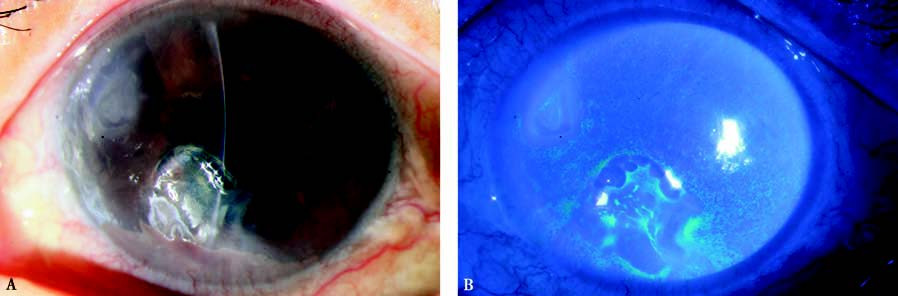
Figure 1 Bullous keratopathy
A. The corneal epithelium exhibits a hazy appearance and bullae of varying sizes.
B. Fluorescein sodium staining reveals multiple bulla-like lesions in the corneal epithelium.
Treatment
Mild cases may be managed with topical hyperosmotic agents and medications that protect and lubricate the cornea. Antibiotic eye drops are used to prevent infection in cases with epithelial defects. For persistent symptoms or significant visual impairment, corneal endothelial transplantation or penetrating keratoplasty may be considered to alleviate pain and restore vision. Other approaches, such as stromal cautery, may be used for symptomatic relief.