Epidemic keratoconjunctivitis is a highly contagious contact-transmitted disease caused by adenovirus types 8, 19, 29, and 37 (human adenovirus subgroup D). The incubation period is 5–7 days. The condition is more common in adults aged 20–40 years and primarily spreads through direct human contact or contamination.
Clinical Manifestations
The onset is sudden with severe symptoms, affecting both eyes. The primary symptoms include eye redness, pain, photophobia, and watery discharge. During the early stage, one eye is often affected first, followed by involvement of the other eye within a few days. During the acute phase, eyelid swelling and conjunctival hyperemia with edema are observed. Within 48 hours, follicles and subconjunctival hemorrhages develop. The formation of pseudomembranes (or sometimes true membranes) can lead to flat scarring and symblepharon. A few days after onset, the cornea may show diffuse punctate epithelial lesions, which merge into larger, rough epithelial infiltrates within 7–10 days. After two weeks, subepithelial infiltrates develop, primarily in the central cornea, with normal corneal sensitivity.
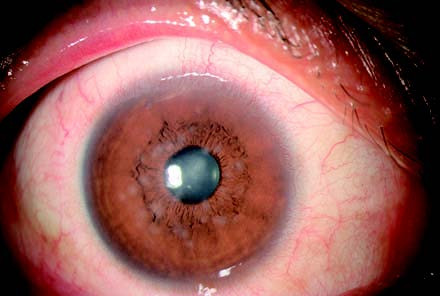
Figure 1 Adenoviral keratoconjunctivitis
In 3–4 weeks, the subepithelial infiltrates increase in intensity, with uniform size and shape, ranging from a few to several dozen. These subepithelial infiltrates result from a delayed hypersensitivity reaction, characterized by lymphocytic infiltration in the anterior limiting and anterior stromal layers. This represents an immune response to viral antigens and may persist for several months or even years, gradually resolving. Conjunctival inflammation generally lasts up to 3–4 weeks. Enlargement and tenderness of the preauricular lymph nodes, often more pronounced on the side first affected by ocular involvement, are distinguishing features compared to other types of conjunctivitis. Mild cases or early-stage disease may lack these signs. Systemic symptoms such as fever, pharyngitis, otitis media, and diarrhea may occur, particularly in children.
Diagnosis
Acute follicular conjunctivitis and subepithelial corneal infiltrates, which appear in the later stages of inflammation, are hallmark features. Conjunctival scrapings typically show a large number of mononuclear cells, and in the presence of pseudomembranes, an increased number of neutrophils is observed.
Treatment and Prevention
Local cold compresses and vasoconstrictors can help alleviate symptoms. During the acute phase, antiviral drugs may be used to inhibit viral replication, including interferon eye drops, 0.1% acyclovir, or 0.15% ganciclovir eye drops, administered hourly. If bacterial infection coincides, antibiotics are added to the treatment regimen. In cases involving severe membrane or pseudomembrane formation, epithelial, or subepithelial keratitis, corticosteroid eye drops may be considered. The frequency of corticosteroid use should be gradually reduced to once daily or every other day after the condition is controlled to avoid recurrence, while also monitoring for corticosteroid-related side effects.
Efforts to reduce transmission involve limiting contact between infected individuals and others. All instruments in contact with the infected patient must be thoroughly cleaned and disinfected. Patients are advised not to touch their eyelids or tears and to practice frequent handwashing.