Thyroglossal cyst and fistula are the most common congenital disorders of the neck, associated with abnormal embryological development of the thyroglossal duct. During embryogenesis, failure of the thyroglossal duct to degenerate completely or partial degeneration leads to the formation of thyroglossal cysts and fistulas. Thyroglossal cysts are mostly located below the hyoid bone. Thyroglossal fistulas can be classified into two types: complete and incomplete.
In complete fistulas, the external opening is located on the skin surface along the anterior midline of the neck or slightly to one side, while the internal opening is at the foramen cecum of the tongue. The fistulous tract extends from the internal opening, passing either above, below, or through the hyoid bone, connecting to the cyst or the external opening. In incomplete fistulas, an internal opening is absent.
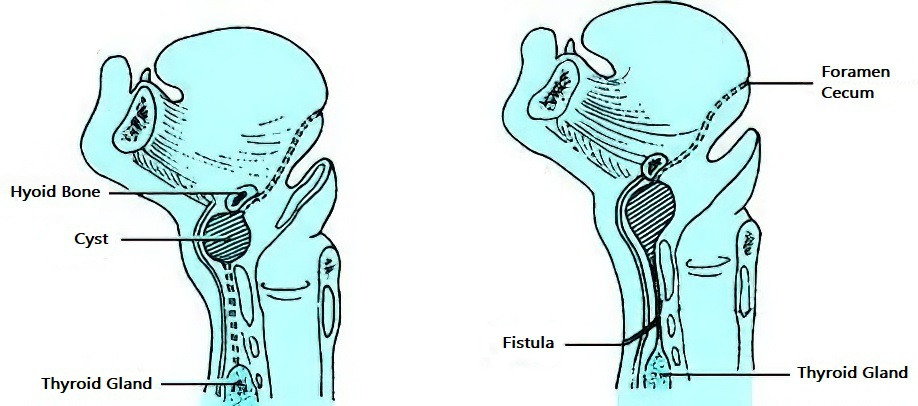
Figure 1 Schematic diagram of thyroglossal cyst formation
Clinical Manifestations
Thyroglossal Cysts
The size of the cysts can vary and is generally asymptomatic, often discovered incidentally or during routine physical examination. The cyst is round, smooth, well-demarcated, non-adherent to surrounding tissues and skin, painless, and soft to moderately firm, with a cystic consistency. It moves up and down with swallowing. In some cases, a cord-like structure may be palpated above the cyst. When complicated by infection, the cyst enlarges rapidly and may be associated with localized pain and tenderness. In cases of recurrent infection, adhesions between the cyst and surrounding tissues or skin may be detected upon palpation.
Thyroglossal Fistula
The external opening is located in the anterior midline of the neck or slightly to one side. The opening is small, often discharging secretions. When secondary infection occurs, redness and swelling can develop around the opening, and purulent discharge may be present.
Diagnosis and Differential Diagnosis
A preliminary diagnosis can be made if a cyst or fistula is located in the anterior midline of the neck and exhibits upward and downward movement with swallowing. For complete fistulas, injecting methylene blue into the external opening and observing whether it appears at the foramen cecum can further confirm the diagnosis. Ultrasonography (B-mode ultrasound) is helpful in diagnosing cystic lesions. Thyroglossal cysts should be differentiated from the following conditions:
Dermoid Cysts
Dermoid cysts are congenital and located in the anterior midline of the neck. Unlike thyroglossal cysts, dermoid cysts are adherent to the skin and do not move with swallowing.
Submental Lymphadenitis
Submental lymphadenitis often presents with inflammation in adjacent tissues, such as the periodontium, mandible, or lower lip. The mass is firm, tender, and does not move with swallowing.
Ectopic Thyroid
Ectopic thyroid tissue is often located at the base of the tongue, though it may rarely be found in the anterior midline of the neck, making it easy to confuse with a thyroglossal cyst. Ultrasonography and radionuclide imaging using 131I can help differentiate these conditions. It is also essential to ensure the presence of normal thyroid tissue in its usual location in the neck.
Treatment
Complete excision of the cyst along with the fistulous tract is recommended to prevent postoperative recurrence.