Vocal nodules refer to symmetric nodular elevations at the junction of the anterior and middle thirds of both vocal cords.
Etiology
Vocal nodules are commonly observed in individuals with professional voice use or excessive voice strain, such as singers, teachers, individuals in occupations requiring frequent loud speaking, and children. It is currently believed that prolonged vocal overuse or improper voice use is a significant cause of this condition.
The anterior 2/3 of the vocal cord is the membranous portion, while the posterior one-third is the cartilaginous portion (the arytenoid cartilage). The midpoint of the membranous portion, at the junction of the anterior and middle thirds, exhibits the greatest vibratory amplitude during phonation. Excessive or improper vocal use can lead to the formation of nodules at this location.
Pathology
Vocal nodules can be classified into three stages based on their developmental process:
Early Stage
The stroma shows edema, with vascular proliferation and dilation, covered by normal squamous epithelium. The appearance is similar to a small polyp, and the pathological changes resemble that of a polyp.
Intermediate Stage
Fibrosis and hyaline degeneration develop in the stroma, but the surface remains covered by normal squamous epithelium. At this stage, the nodule appears more firm.
Late Stage
The stroma exhibits changes similar to the intermediate stage, but the epithelial surface becomes thickened and keratinized. There may also be thickening and incomplete keratinization of the prickle cell layer. As a result, the nodule appears pale in color.
Symptoms
The primary symptom is hoarseness. In the early stage, hoarseness is mild, presenting as a slight coarseness or a near-normal voice, with fatigue occurring after prolonged use of the voice. Early symptoms are intermittent and may vary between better and worse. Gradually, the condition worsens, transitioning to persistent hoarseness that can ultimately affect work.
Examination
Laryngoscopy reveals symmetric nodular elevations at the junction of the anterior and middle thirds of both vocal cords. In cases with a short disease history, early nodules appear pink and polyp-like. In cases with a longer duration, the nodules appear white, smooth, and small. During phonation, the nodules from both sides touch each other, preventing complete closure of the glottis.
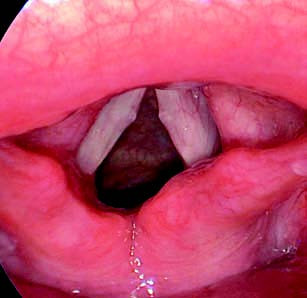
Figure 1 Vocal nodules
Diagnosis
The diagnosis primarily relies on the symptom of persistent hoarseness. Laryngoscopic findings of symmetric nodular elevations at the junction of the anterior and middle thirds of both vocal cords further confirm the diagnosis.
Treatment
Voice Rest
Early-stage vocal nodules may resolve spontaneously with sufficient voice rest. In children, vocal nodules often disappear during puberty.
Surgical Treatment
For cases unresponsive to conservative treatment, surgical removal of the nodules can be performed under local surface anesthesia using a fiberoptic (or electronic) nasopharyngoscope or under general anesthesia with a laryngoscope during microlaryngeal surgery. Postoperatively, appropriate voice rest and nebulized therapy are recommended.
Voice Training and Therapy
Techniques to improve and optimize voice use can be utilized.