Acute epiglottitis, also known as acute supraglottic laryngitis, is a severe and life-threatening infection that can lead to laryngeal obstruction and asphyxiation death. It is more common in adults, occurring in all seasons but more frequently in winter and spring.
Etiology
Infections
Infection is the primary cause of this condition. Pathogens include Haemophilus influenzae type B, Staphylococcus, Streptococcus, and Streptococcus pneumoniae. Mixed infections with viruses or infections secondary to trauma or foreign bodies can also occur.
Hypersensitivity Reactions
Reactions to specific allergens can lead to hypersensitivity-induced inflammation of the epiglottis. This may develop secondary bacterial or viral infections, or it may manifest as isolated inflammation causing epiglottic swelling.
Others
Acute epiglottitis can be caused by foreign bodies, trauma, inhalation of toxic gases, accidental ingestion of chemical agents, or radiation injuries.
Pathology
Acute Catarrhal Type
This manifests as diffuse congestion and swelling of the epiglottic mucosa. Due to the loose submucosal tissue on the lingual surface of the epiglottis, swelling is more pronounced in this area.
Acute Edematous Type
In cases of hypersensitivity-induced inflammation, the mucosal changes are predominantly edematous. When swelling is severe, the epiglottis may appear ball-shaped, significantly increasing the risk of laryngeal obstruction.
Acute Ulcerative Type
This rare form progresses rapidly and is severe. Inflammation spreads to the submucosal layers and glands, leading to local mucosal ulcers. Bleeding may occur if blood vessels are damaged.
Clinical Manifestations
Systemic Symptoms
The onset is sudden, with chills, fever, and body temperatures typically ranging between 38–39°C. Symptoms may be more severe in elderly individuals or children, including lethargy and pale complexion.
Local Symptoms
Many patients experience severe throat pain, which worsens during swallowing. In severe cases, even saliva may be difficult to swallow. Speech becomes muffled and unclear. Significant epiglottic swelling can cause inspiratory dyspnea, and in extreme cases, suffocation. The vocal cords are usually not affected, and hoarseness is rare.
Examination
Patients often appear acutely ill, with severe cases showing signs of respiratory distress. Oropharyngeal examination is usually unremarkable. Indirect laryngoscopy reveals marked congestion and swelling of the epiglottis, which may appear ball-shaped in severe cases. In cases of epiglottic abscesses, yellow-white purulent spots may be seen on the red swollen mucosal surface. The structures of the larynx, such as the ventricular folds and vocal cords, are often obscured by the swollen epiglottis.
Diagnosis
For adult patients reporting severe throat pain that worsens with swallowing and showing no obvious abnormalities during oropharyngeal examination, acute epiglottitis should be suspected. Indirect laryngoscopy confirms the diagnosis by revealing a swollen, congested epiglottis.
In young children, whose epiglottis is anatomically higher, the diagnosis is made when redness and swelling of the epiglottis are observed immediately after depressing the tongue with a spatula.
Flexible (electronic) nasopharyngolaryngoscopy can confirm the diagnosis and determine the presence of acute epiglottitis. Swelling of the lingual surface of the epiglottis often obscures the glottic opening.
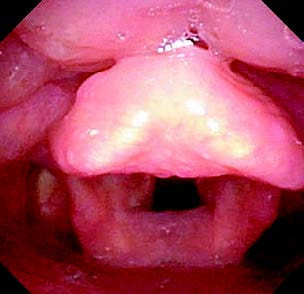
Figure 1 Acute epiglottitis
Treatment
Acute epiglottitis tends to progress rapidly. Early diagnosis, close monitoring of respiratory status, and timely treatment are crucial to alleviating respiratory distress.
Symptomatic Treatment
Addressing respiratory distress is the most critical aspect of treatment. For patients with grade 3 laryngeal obstruction, preparations for tracheotomy are necessary. In cases of acute hypersensitivity-induced epiglottitis accompanied by episodes of suffocation, the swollen mucosa around the glottis may obstruct the airway, making oral intubation or rigid tracheoscopy difficult, with a low likelihood of success. If a tracheotomy cannot be performed promptly, emergency cricothyrotomy may be required. Once the patient's breathing stabilizes, a conventional tracheotomy can be performed.
Etiological Treatment
For infection, systemic administration of adequate antibiotics is essential. If an epiglottic abscess forms, incision and drainage can be performed under laryngoscopy.
Identified cases of hypersensitivity-induced epiglottitis in adults should be managed with effective antiallergic therapy.
Patients whose symptoms do not improve or worsen within a short period after treatment should be informed of the severity of their condition. Preventative tracheotomy may be performed regardless of the extent of respiratory obstruction.
Supportive Care
Patients with eating difficulties benefit from intravenous fluid supplementation and other supportive therapies.