Etiology
Hasty eating may lead to accidental swallowing of objects such as fish bones, meat bones, or fruit pits.
Children often place objects in their mouths, and when crying, laughing, or falling, foreign bodies may inadvertently fall into the pharynx.
Individuals with mental disorders, those in a coma, intoxicated, or under incomplete anesthesia may experience accidental ingestion.
Older adults with loose dentures may have them dislodge and fall into the pharynx.
Swallowing reflexes may become sluggish or absent due to central nervous system disorders, causing food boluses to obstruct the pharynx.
Individuals attempting suicide may intentionally ingest foreign objects.
During medical procedures, items such as hemostatic cotton balls or gauze strips may accidentally be left in the nasopharynx or tonsillar fossae, leading to the formation of foreign bodies.
Clinical Manifestations
A pricking sensation or pain in the pharynx is often associated with foreign bodies, particularly during swallowing, and the location is usually fixed.
Mucosal injury caused by foreign bodies may result in a small amount of bleeding, observed as blood-streaked saliva.
Larger foreign bodies lodged in the pharynx or larynx may cause difficulty swallowing and breathing.
Most foreign bodies are located in the tonsillar fossae, tongue base, vallecula, or piriform sinus. Nasopharyngeal foreign bodies are rare and may occur if food particles or tablets are forced into the area during vomiting or coughing.
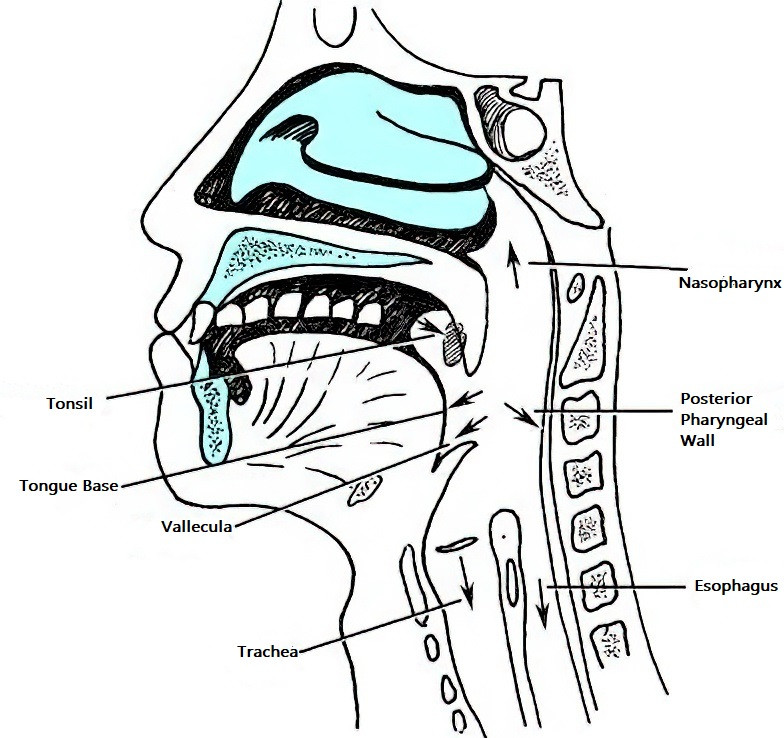
Figure 1 Common locations and possible directions of lodgment for pharyngeal foreign bodies
Diagnosis
A diagnosis of pharyngeal foreign bodies is often established through patient history, inspection of the oropharynx, and examination using a nasopharyngoscope or indirect laryngoscope. X-rays and CT scans can also help detect foreign bodies of different materials and determine their shape, size, and location.
Treatment
Foreign bodies in the oropharynx, such as fish bones or bamboo splinters, can typically be removed using forceps. Foreign bodies located in areas such as the tongue base, vallecula, or piriform sinus can be extracted using foreign body forceps under indirect laryngoscopy or fiberoptic laryngoscopy. Larger foreign bodies causing pharyngeal obstruction and breathing difficulties may require immediate lifting of the tongue base and removal with an oval forceps. Antibiotics are administered to control infections if they have already developed, followed by removal of the foreign body. For cases involving foreign bodies that penetrate the pharyngeal wall and result in retropharyngeal or parapharyngeal abscesses, drainage via an oral or lateral cervical incision and concurrent removal of the foreign body may be performed as needed.