Acute tonsillitis refers to acute non-specific inflammation of the palatine tonsils, often accompanied by varying degrees of inflammation of the pharyngeal mucosa and lymphoid tissue. It is a common disorder of the throat, frequently occurring in children and young adults. The condition tends to be more prevalent during seasonal temperature changes in spring and autumn.
Etiology
The primary causative agent of this condition is beta-hemolytic streptococcus. Other pathogens such as non-hemolytic streptococcus, staphylococcus, pneumococcus, Haemophilus influenzae, adenovirus, rhinovirus, and herpes simplex virus may also cause the disease. Cases of mixed bacterial and viral infections are common. Recent studies have also identified infections caused by anaerobic bacteria and an increasing prevalence of gram-negative bacterial infections.
Certain pathogens normally reside in the pharynx and tonsillar crypts, and inflammation develops when the host's resistance decreases, allowing these pathogens to proliferate, produce toxins, and damage the crypt epithelium. This can lead to bacterial invasion of the tonsillar tissue. Factors such as cold exposure, humidity, overexertion, excessive smoking or alcohol consumption, irritants such as harmful gases, and chronic upper respiratory diseases may trigger the condition. The pathogens associated with acute tonsillitis may be transmitted through droplets or direct contact. Outbreaks are usually sporadic but may occur in groups, such as within military units, factories, or schools.
Pathology
The condition is generally categorized into three types:
Acute Catarrhal Tonsillitis
This type is often caused by viruses and involves mild inflammation that remains confined to the mucosal surface, with no significant changes in the tonsillar crypts or tissue.
Acute Follicular Tonsillitis
In this type, inflammation extends to the lymphoid follicles within the tonsillar tissue, leading to congestion, swelling, and in some cases, suppuration. Yellowish-white spots may appear beneath the mucous membrane near crypt openings.
Acute Lacunar Tonsillitis
This type is characterized by congestion and swelling of the tonsils. Exudates composed of desquamated epithelium, fibrin, pus cells, and bacteria accumulate within the crypts and may emerge through crypt openings. The exudates may form into patches of membranous-like structures that can be easily wiped off.
Clinically, acute tonsillitis is often classified into two categories: acute catarrhal tonsillitis and acute suppurative tonsillitis. The latter includes both acute follicular tonsillitis and acute lacunar tonsillitis.
Clinical Manifestations
The symptoms of the different types of tonsillitis are similar. General and localized symptoms are mild in cases of acute catarrhal tonsillitis.
Systemic Symptoms
Systemic symptoms are more commonly observed in acute suppurative tonsillitis. The onset is rapid, with manifestations such as chills, high fever, headache, decreased appetite, fatigue, generalized discomfort, and constipation. In children, febrile seizures, vomiting, and lethargy may also occur due to high fever.
Local Symptoms
Severe sore throat is the primary symptom, often radiating to the ears, accompanied by difficulty in swallowing. Enlargement of the submandibular lymph nodes may occur, sometimes causing discomfort when turning the head. Staphylococcal infections may lead to significant tonsillar swelling, which in young children may result in breathing difficulties.
Examinations
Affected individuals often appear acutely ill. Diffuse congestion of the pharyngeal mucosa, most notably in the palatine arches, can generally be observed. The palatine tonsils are swollen, with yellowish-white pus points on the surface or yellowish-white to grayish-white bean curd-like exudates in the crypt openings. These exudates may form into patches resembling a pseudomembrane. Enlargement of the submandibular lymph nodes is also common.

Figure 1 Acute tonsillitis
Acute congestion of both palatine arches and tonsils is observed. The tonsils are bilaterally enlarged to Grade II, with scattered pus points visible at the openings of the tonsillar crypts.
Diagnosis and Differential Diagnosis
Diagnosis is typically straightforward when based on the characteristic clinical manifestations. Differential diagnosis is necessary to distinguish acute tonsillitis from conditions such as pharyngeal diphtheria, Vincent's angina, and pharyngitis caused by certain hematological disorders.
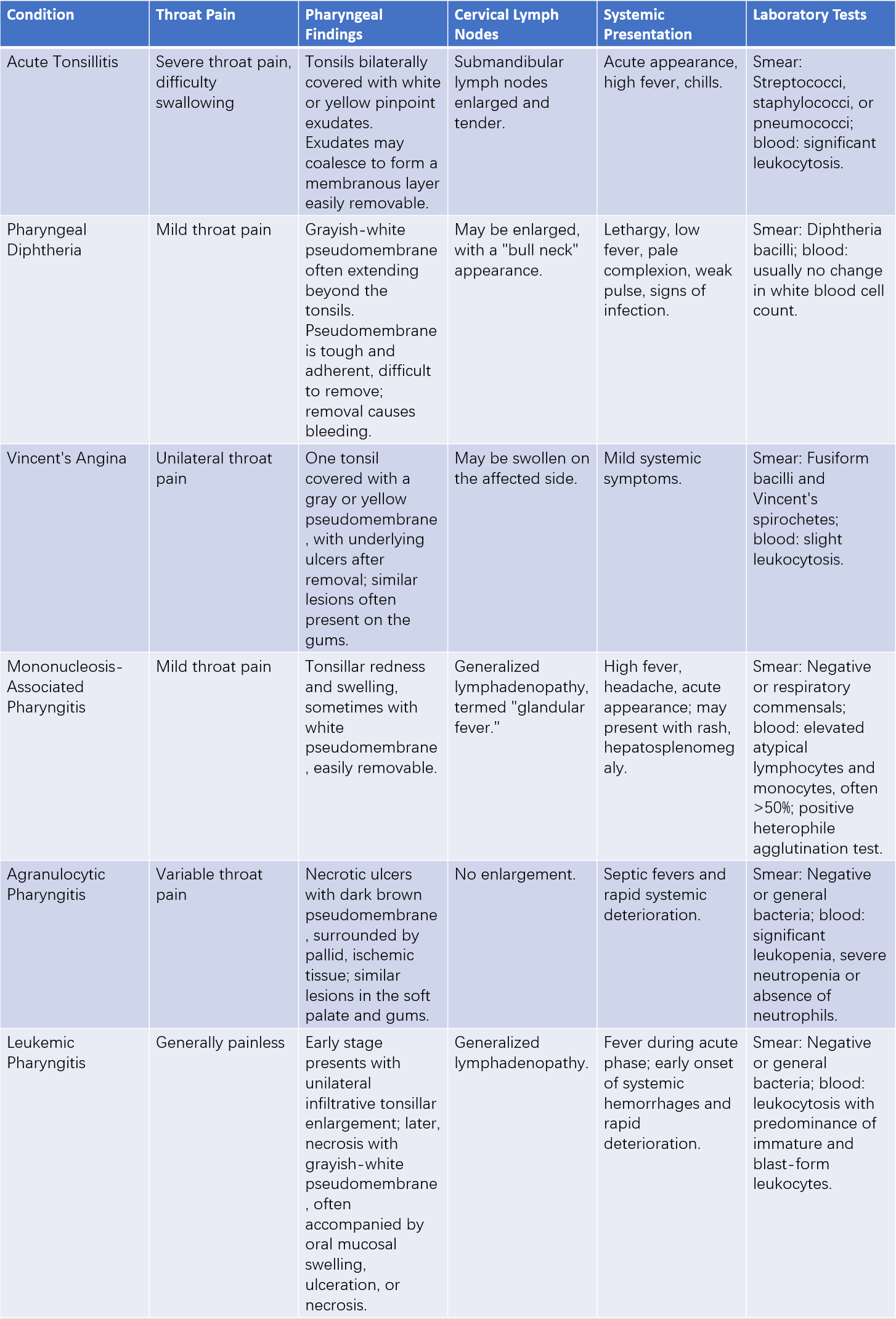
Table 1 Differential diagnosis of acute tonsillitis
Complications
Local Complications
Inflammatory involvement of neighboring tissues often leads to peritonsillar abscesses. Other possible complications include acute otitis media, acute rhinitis, sinusitis, acute laryngitis, acute lymphadenitis, and parapharyngeal abscess.
Systemic Complications
Acute tonsillitis may result in a variety of systemic conditions, such as acute rheumatic fever, myocarditis, acute nephritis, acute arthritis, and acute osteomyelitis. The precise mechanisms of these complications remain under investigation, but they are generally thought to involve Type III hypersensitivity reactions between target organs and streptococcal antigens.
Treatment
General Therapy
Given the contagion risk of this disease, patients require appropriate isolation. Measures include bed rest, a liquid diet, increased fluid intake, improved nutrition, and relief of constipation. When sore throat is severe or high fever is present, antipyretic and analgesic medications can be administered.
Antibiotic Therapy
Antibiotics represent the mainstay of treatment, with penicillin being the preferred choice. The route of administration depends on the severity of the disease. If there is no improvement after 2–3 days of treatment or if fever persists, reevaluation of the condition is necessary, and alternative antibiotic options should be considered. Glucocorticoids may be used as needed.
Local Treatment
Local treatments typically involve gargling with solutions such as compound borax solution, compound chlorhexidine gargles, or 1:5,000 furacilin solution. Antimicrobial gargling solutions provide additional benefits.
Surgical Treatment
Acute tonsillitis has a tendency to recur. Tonsillectomy is recommended in individuals with complications once the acute inflammation has resolved.