Nasal endoscopic surgery (NES) is one of the hallmark techniques of modern rhinology. It involves performing procedures in regions such as the nasal cavity, paranasal sinuses, skull base, and orbit with the aid of nasal endoscopes, surgical instruments, and monitoring systems. Endoscopic sinus surgery serves as the foundation of NES and is primarily used for treating chronic rhinosinusitis with nasal polyps, benign or malignant tumors of the sinuses, and nasal cavity or sinus foreign bodies. It also serves as a preparatory step for skull base or orbit-related surgical procedures. Sinus surgery can be performed under either local or general anesthesia, depending on the patient’s overall condition.
There are two basic surgical approaches in endoscopic sinus surgery, with the most commonly used being the Messerlinger technique.
Messerlinger Technique
This is an anterior-to-posterior approach, involving the following steps:
- Resection of the uncinate process.
- Opening of the ethmoid bulla.
- Removal of the basal lamella of the middle turbinate to access the posterior ethmoid sinuses.
- Enlargement of the sphenoid sinus ostium via the sphenoethmoidal recess.
- Widening of the posterior fontanelle to expand the maxillary sinus ostium.
- Cleaning of the frontal recess cells and opening the frontal sinus.
The main surgical steps are as follows:
Resection of the Uncinate Process
The resection of the uncinate process is the initial step in sinus opening, which helps expand the surgical field and facilitates subsequent procedures. The uncinate process attachment on the lateral nasal wall is identified using a dissector or sickle knife to determine the incision trajectory. A dissector is then inserted into the vertical portion of the uncinate process, penetrating the mucoperiosteum to reach the ethmoidal infundibulum. The mucoperiosteum is incised in an arc from the anterior superior to the posterior inferior direction, extending to the horizontal portion of the uncinate process. The uncinate process is detached medially, and its upper and lower sections are cut with middle turbinate scissors. Upon removal of the uncinate process, the posterior ethmoid bulla becomes visible. Care should be taken to avoid inserting the dissector or sickle knife too deeply laterally, as this may damage the lamina papyracea.
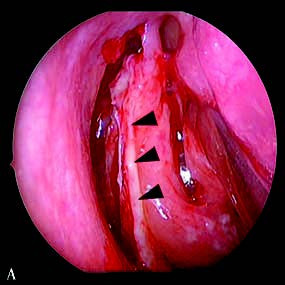
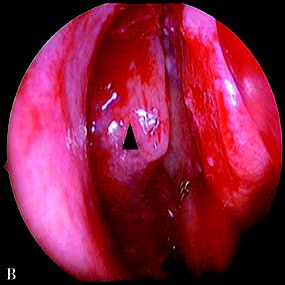
Figure 1 Uncinate process resection
A. The arrow indicates the uncinate process (already incised and medially separated, with polypoid changes on its surface mucosa);
B. The arrow indicates the ethmoid bulla.
Opening of the Ethmoid Sinuses
The opening of the ethmoid air cells follows a sequence from inferomedial to superolateral. The ethmoid bulla is incised and gradually removed using mucosal nibblers or a dissector, exposing the basal lamella of the middle turbinate. The basal lamella is an important landmark separating the anterior and posterior ethmoid sinuses. An incision is made at the junction of the vertical and horizontal portions of the basal lamella, followed by the stepwise removal of the lamella to enter the posterior ethmoid sinuses. The posterior ethmoid air cells are cleared, and surgical landmarks such as the superior meatus, superior turbinate, and basal lamella of the superior turbinate are identified. Gentle handling is required near the lamina papyracea and the skull base, while damage to the cribriform plate should be avoided when operating on the root of the middle turbinate. When an Onodi cell is present, the optic nerve canal should be carefully identified to avoid accidental injury.
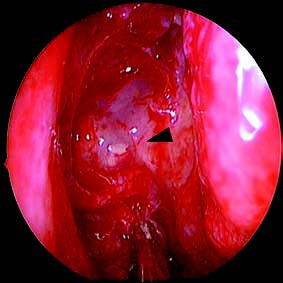
Figure 2 The area indicated by the arrow represents the basal lamella of the middle turbinate, which serves as the boundary between the anterior and posterior ethmoid sinuses.
Opening of the Sphenoid Sinuses
The natural ostium of the sphenoid sinus is located in the sphenoethmoidal recess, about 1–1.5 cm above the superior border of the choana and in the upper-middle third of the anterior wall of the sphenoid sinus. The posterior-inferior portion of the superior turbinate is excised to fully expose the sphenoethmoidal recess. A dissector or probe is used to locate the natural ostium. If the sinus ostium is already wide open with smooth mucosa, further enlargement may not be necessary. However, significant mucosal lesions warrant enlargement of the ostium downward and outward. Downward enlargement requires caution to avoid damaging the posterior septal branches of the sphenopalatine artery, which, if injured, should be treated with electrocautery to achieve hemostasis. Outward enlargement requires attention to avoid injury to the orbital apex, optic nerve canal, and carotid artery canal.
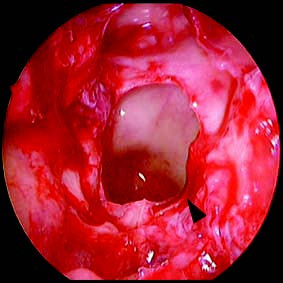
Figure 3 Enlarged sphenoid sinus ostium (arrow)
Opening of the Maxillary Sinuses
A curved suction tube or probe is used to identify the maxillary sinus opening, located below the ethmoidal infundibulum in the region where the maxillary line meets the lower border of the inferior turbinate. Once identified, the anterior fontanelle is widened using angled forceps, taking care to avoid damaging the nasolacrimal duct. Posteriorly, the posterior fontanelle and the tail of the uncinate process are excised with straight nibblers. The extent of maxillary sinus opening depends on the nature and severity of the disease affecting the surrounding mucosa and the sinus cavity itself. Normal mucosa is preserved, and excessive exposure of bone is avoided to facilitate recovery of the mucociliary clearance function.
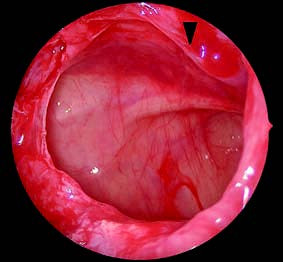
Figure 4 Enlarged maxillary sinus ostium (arrow)
Opening of the Frontal Sinus
The frontal sinus can be opened using a 0° endoscope through the nasal infundibulum or a 70° endoscope through the frontal recess. Preoperative CT imaging helps determine the development and distribution of the frontoethmoidal air cells, the anatomical relationship between the nasal infundibulum and the uncinate process, and the drainage pathway of the frontal sinus. The frontoethmoidal air cells are removed, and the frontal sinus ostium is widened. Protection of the mucosa around the frontal sinus opening is ensured to prevent postoperative scarring and obstruction.
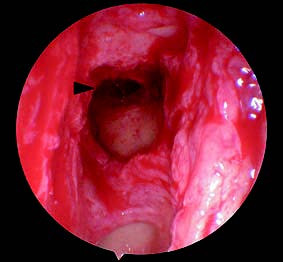
Figure 5 Enlarged frontal sinus ostium (arrow)
Nasal Cavity Packing
Nasal cavity packing is performed for hemostasis, shaping, and promoting surgical wound healing. Absorbable packing materials are commonly used to minimize postoperative discomfort associated with packing removal.
Wigand Technique
The Wigand technique is a posterior-to-anterior approach. The main steps include:
- Resection of the inferior part of the middle turbinate.
- Enlargement of the sphenoid sinus opening through the sphenoethmoidal recess.
- Progressive opening of the posterior ethmoid and anterior ethmoid air cells.
- Widening of the posterior fontanelle and maxillary sinus opening.
- Clearing of the frontal recess air cells.
- Opening of the frontal sinus.
This approach is more complex as it requires partial removal of the middle turbinate and is therefore less commonly used. It is mainly indicated for lesions in the posterior ethmoid or sphenoid sinus regions.