The nasal region is a relatively prominent area of the face, making it susceptible to trauma. The nasal bone is located above the piriform aperture, connecting with surrounding bones on either side of the midline. When subjected to an external force, fractures of the nasal bone (fracture of nasal bone) often occur. Due to the anatomical structure, with the upper part of the nasal bone being narrow and thick and the lower part being wide and thin, fracture typically involves collapse of the lower portion of the nasal bone and downward displacement. Nasal bone fractures can be isolated or combined with fractures of the maxillofacial bones and the cranial base. For example, injuries to the nasal root and medial canthus may result in fractures involving the nasal bone, ethmoid bone, and orbital walls, forming a nasoethmoidal-orbital complex fracture.
In children, nasal bone fractures are more challenging to diagnose than in adults due to the small size of the external nose and nasal bone, as well as the frequent presence of hematomas, bruising, and swelling. Since most of the nasal support structure in children is composed of cartilage and partially ossified, trauma often leads to incomplete fractures or greenstick fractures, which may occur without significant displacement.
Etiology
Nasal bone fractures are the most common type of fracture in the maxillofacial region. Common causes include impact to the nasal region, sports-related injuries, personal accidents, and traffic collisions.
Clinical Manifestations
Typical symptoms and signs include localized pain, swelling, nasal mucosa laceration resulting in epistaxis, deformities of the nose and surrounding area, such as widened, deviated, or collapsed nasal bridge leading to saddle nose.
The presentation varies depending on the direction and intensity of the force applied. In cases of laceration to the nasal mucosa, periosteum, and mucosa of the nasolacrimal ducts, air may enter the subcutaneous tissue of the eyelids or cheeks, causing subcutaneous emphysema. Trauma-induced nasal septum deviations, dislocations, and hematomas may lead to nasal congestion and other symptoms.
Palpation of the nasal region may reveal nasal bone collapse and crepitus, while subcutaneous emphysema may produce crackling sounds. Swelling can often mask nasal deformities within hours of the injury. Observation of external nasal deformities is clearer after swelling subsides, typically around one week after injury.
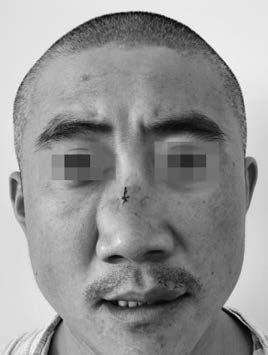
Figure 1 External nasal deformity in a patient with nasal bone fracture
Auxiliary examinations include lateral X-rays of the nasal bone to identify transverse fracture lines and vertical displacement. CT scans can provide precise information regarding the presence, location, type of fractures, and potential involvement of surrounding tissues.
Diagnosis
Diagnosis is generally based on the patient’s history, clinical examination, and imaging studies such as nasal bone X-rays in anteroposterior and lateral views or CT scans. For complex injuries caused by traffic accidents or high falls, associated maxillofacial and cranial base fractures should be identified.
Treatment
Management of nasal bone fractures is ideally performed within a few hours after the injury, before swelling develops. It is generally recommended to complete treatment within two weeks to prevent deformity during healing.
For closed nasal bone fractures, treatment varies depending on the type:
- Non-displaced fractures do not require repositioning.
- Displaced fractures can be repositioned under nasal mucosal anesthesia or anterior ethmoidal nerve block if necessary, using internal or external techniques. Care is taken to ensure instruments used within the nasal cavity do not exceed the line between the medial canthi to avoid damage to the cribriform plate.
- Open nasal bone fractures ideally undergo primary wound debridement, suturing, and fracture repositioning. In cases of nasal septum injuries leading to deviation or dislocation, open repositioning is appropriate.
- Nasal septum hematomas and abscesses are treated surgically as early as possible to prevent cartilage necrosis and secondary infections.
- Comminuted nasal bone fractures may require stabilization through suturing, fixation (e.g., local drilling, through-and-through sutures, or metal plate fixation), as well as nasal cavity packing. Nasal packing is typically removed within 48–72 hours.
- Complex nasoethmoidal-orbital fractures, often associated with severe craniofacial injuries, may necessitate open repositioning. Multiple metal plates can be used to align and stabilize fragmented nasal bones and surrounding structures, or nasal airway drainage tubes can be utilized for compressive fixation.