Secretory otitis media (SOM) is a non-suppurative inflammatory disease of the middle ear characterized primarily by conductive hearing loss and the presence of effusion in the tympanic cavity. It is more common in the winter and spring and is one of the leading causes of hearing loss in both children and adults. Historically, this condition has been referred to by various names, including non-suppurative otitis media, exudative otitis media, catarrhal otitis media, serous otitis media, seromucous otitis media, middle ear effusion, and glue ear. SOM can be classified as acute SOM and chronic SOM. An acute course lasts up to 8 weeks, while cases persisting beyond 8 weeks are considered chronic SOM. Chronic SOM often develops from unresolved acute SOM but can also have a slow onset without a history of acute otitis media.
Etiology
SOM is often associated with upper respiratory tract infections and may also occur after radiotherapy for head and neck tumors. Any condition that causes systemic or local immune suppression, such as aging, childhood, excessive fatigue, and overuse of tobacco and alcohol, can predispose individuals to this condition. The primary causes include Eustachian tube dysfunction, local middle ear infections, and allergic reactions.
Eustachian Tube Dysfunction
Mechanical Obstruction
Common causes include adenoid hypertrophy in children, hypertrophic rhinitis, nasopharyngeal tumors or lymphoid hyperplasia, and prolonged blockage of the posterior nasal cavity or nasopharynx.
Functional Impairment
Weak contraction of the muscles responsible for opening and closing the Eustachian tube, reduced cartilage elasticity, and collapse of the cartilaginous portion of the tube can lead to dysfunction. In children, the Eustachian tube is shorter, wider, and more horizontal, making it easier for infections from the nose and throat to spread to the middle ear, which explains the higher incidence of SOM in children. In patients with cleft palate, the lack of a midline attachment point for palatal muscles results in poor contraction and inability to actively open the Eustachian tube, increasing susceptibility to SOM.
Dysfunction of the mucociliary clearance system of the Eustachian tube mucosa, including impaired surface tension and allergic reactions, is another important pathogenic factor. This is also a major mechanism behind SOM following radiotherapy for head and neck tumors.
Local Middle Ear Infection
Studies have found that bacterial cultures of middle ear effusion are positive in 1/3 - 1/2 of cases, with Haemophilus influenzae and Streptococcus pneumoniae being the most common pathogens. Bacteriological, histological, and clinical evidence suggests that SOM may represent a mild or low-grade bacterial infection of the middle ear. Bacterial endotoxins may play a role in the disease process, particularly in the progression to chronic SOM.
Allergic Reactions
The immature immune system in children may partly explain the higher incidence of SOM in this population. Inflammatory mediators such as prostaglandins, bacteria-specific antibodies, immune complexes, complement system components, and lysozyme enzymes have been detected in middle ear effusion. This suggests that chronic SOM may involve an immune-mediated pathological process triggered by infection.
Barotrauma
Rapid changes in atmospheric pressure, such as during flying or diving, can also cause this condition, which is clinically referred to as barotraumatic otitis media.
Pathology
When Eustachian tube dysfunction prevents air from entering the middle ear, the gas within the middle ear is gradually resorbed, creating negative pressure. This leads to venous dilation, congestion of the middle ear mucosa, and increased vascular permeability, resulting in the formation of transudate. If the negative pressure persists, the middle ear mucosa undergoes a series of pathological changes, including epithelial thickening, epithelial metaplasia, and transformation of the low pseudostratified columnar epithelium in the anterior tympanic cavity into thickened ciliated epithelium. The simple squamous epithelium in the posterior tympanic cavity transforms into pseudostratified columnar epithelium, with an increase in goblet cells and hypersecretion. Pathological glandular tissue forms in the subepithelial layer, and perivascular infiltration of lymphocytes and plasma cells is observed in the lamina propria.
Middle ear effusion is typically a mixture of transudate, exudate, and secretions, with the dominant component varying depending on the disease stage. When the effusion is extremely viscous, it is referred to as glue ear. This effusion appears grayish-white or brownish-yellow and contains large amounts of proteins such as glycoproteins and nucleoproteins.
Clinical Manifestations
Patients may experience hearing impairment and autophony (increased perception of their own voice). Hearing may improve temporarily when the head is tilted forward or inclined toward the healthy side, as the effusion moves away from the round window.
In children, hearing loss may manifest as delayed responses to sounds or difficulty concentrating, prompting medical consultation. If only one ear is affected and the other ear has normal hearing, the condition may go unnoticed for a long time.
Acute cases may present with ear pain, which can be constant or intermittent. Chronic cases typically have less pronounced ear pain.
Tinnitus is often low-pitched and intermittent, described as crackling, buzzing, or the sound of running water.
Patients may hear a water-bubbling sound in the ear during head movement, yawning, or performing the Valsalva maneuver.
A sensation of blockage or fullness in the ear is common. Pressing on the tragus repeatedly may temporarily alleviate this sensation.
In acute cases, the tympanic membrane may show congestion and retraction in the pars flaccida or the entire membrane. The light reflex may be shortened, distorted, or absent. The handle of the malleus may appear displaced upward and backward, and the short process of the malleus may be more prominent.
With effusion in the tympanic cavity, the tympanic membrane loses its normal luster and may appear pale yellow, orangish red, shiny, or amber. In chronic cases, the tympanic membrane may appear grayish blue or milky white, with dilated microvessels in the tense portion of the membrane.
A hairline shaped fluid level may be visible through the tympanic membrane, with the concave side facing upward. This fluid level remains parallel to the ground regardless of head position. Air bubbles may also be visible through the tympanic membrane, and their number may increase after performing the Valsalva maneuver.
The mobility of the tympanic membrane is restricted.
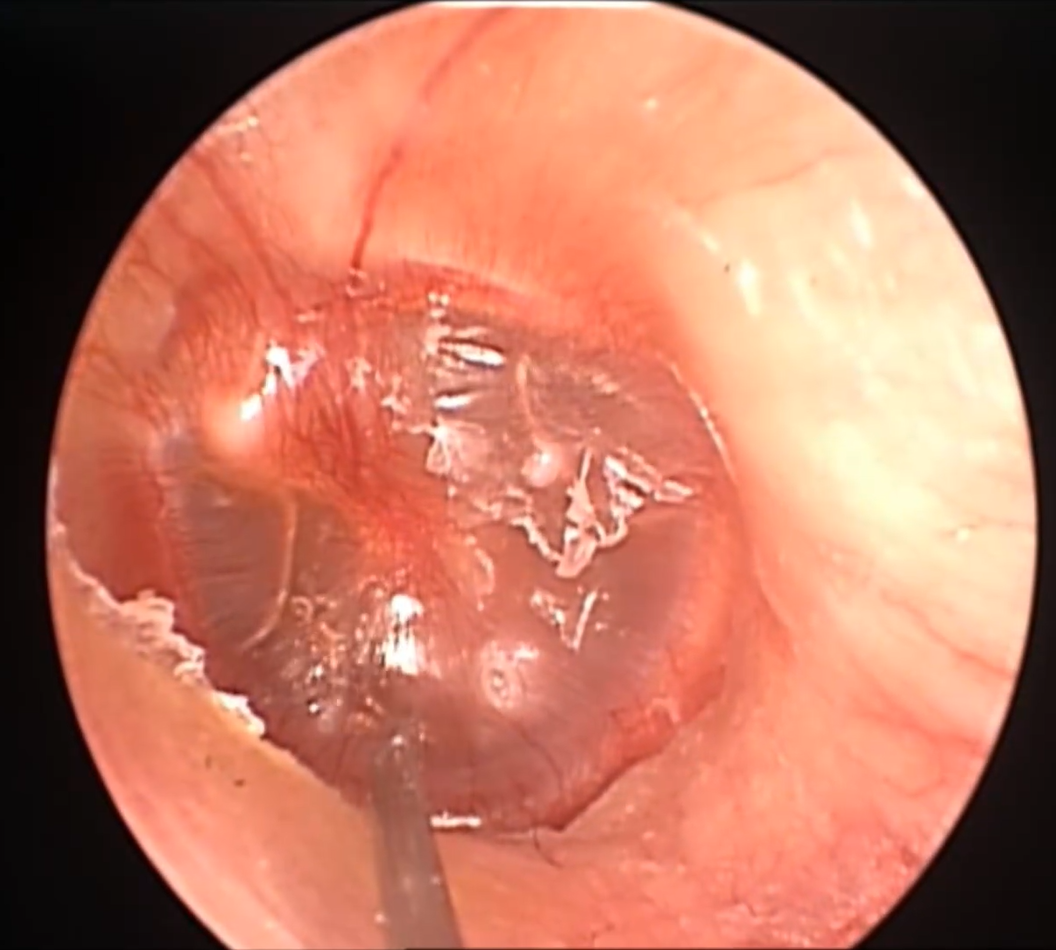
Figure 1 Tympanic effusion in secretory otitis media
Conductive hearing loss is typically observed. The severity of hearing loss varies and can reach up to approximately 40 dB HL in severe cases.
Since the amount of effusion often fluctuates, hearing thresholds may also vary. Hearing loss is generally more pronounced at low frequencies, but high-frequency air conduction and bone conduction may also be affected due to changes in the sound transmission structure of the middle ear and impedance at the two windows. Hearing improves once the effusion is resolved.
A flat tympanogram (Type B) is characteristic of secretory otitis media. A negative pressure curve (Type C) indicates Eustachian tube dysfunction, and some cases may also show middle ear effusion.
CT imaging of the middle ear shows areas of increased density, with CT values typically below 40 HU.
Diagnosis
The diagnosis is generally straightforward based on the patient's history, clinical presentation, and audiological examination findings. Diagnostic tympanocentesis can confirm the diagnosis.
Differential Diagnosis
Nasopharyngeal Tumor
Secretory otitis media may be the initial symptom of nasopharyngeal carcinoma, especially in cases of unilateral chronic SOM in adults. Nasopharyngoscopy, nasopharyngeal CT, or MRI has high diagnostic value.
Cerebrospinal Fluid Otorrhea
In case of temporal bone fracture or congenital defects leading to cerebrospinal fluid leakage into the middle ear without tympanic membrane perforation, the clinical presentation may mimic SOM.
A history of head trauma, laboratory analysis of middle ear fluid, temporal bone CT, and MRI with cerebrospinal fluid imaging can aid in differentiation. Children with cerebrospinal fluid otorrhea may have a history of recurrent meningitis.
Cholesterol Granuloma
Also referred to as idiopathic hemotympanum, this condition may be a late-stage complication of SOM. The tympanic membrane appears blue or bluish-black. Temporal bone CT shows areas of increased density in the tympanic cavity and mastoid.
Glomus Jugulare Tumor
Paragangliomas, such as glomus jugulare tumors and tympanic body tumors, may extend into the tympanic cavity. Patients typically present with pulsatile tinnitus and hearing loss. Larger tumors may cause significant bone destruction, and temporal bone CT can assist in diagnosis.
Prevention
Physical fitness should be strengthened and upper respiratory infections should be prevented.
Health education should be conducted to raise awareness among parents and teachers about this condition.
For children under 10 years old, screening with tympanometry should be considered as needed.
Nasal and nasopharyngeal conditions should be properly treated.
Treatment
The primary goals of treatment are to address the underlying cause, improve middle ear ventilation and drainage, and eliminate middle ear effusion. Conservative treatment is recommended for the first 3 months, with surgical intervention reserved for strictly indicated cases.
In the acute phase, if signs of bacterial infection are present, appropriate antibiotics may be prescribed based on the clinical situation.
Nasal decongestants can be used alternately for nasal drops 3 - 4 times daily, but the duration should not exceed 5 - 7 days. Nasal corticosteroid sprays may also be used as needed.
Mucolytic agents can help improve ciliary drainage function, reduce the surface tension of the Eustachian tube mucosa, and lower the pressure required to open the Eustachian tube.
Oral corticosteroids, such as dexamethasone and prednisone, may be used as adjunctive therapy.
In chronic cases, methods such as the Valsalva maneuver, Politzer balloon inflation, or catheter-assisted inflation can be employed to improve Eustachian tube function.
Tympanocentesis can be performed under local anesthesia in adults and general anesthesia in children. A sterile 22G needle is used to puncture the anteroinferior quadrant of the tympanic membrane to aspirate the effusion from the tympanic cavity.
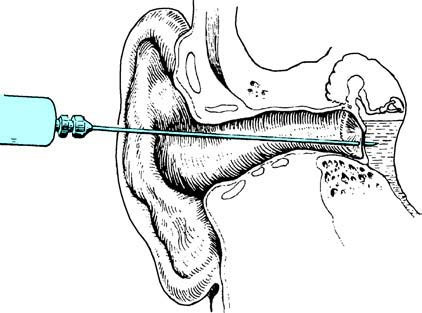
Figure 2 Schematic diagram of the position for tympanocentesis
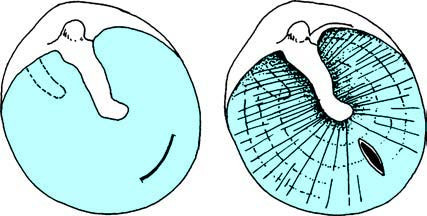
Figure 3 Schematic diagram of tympanotomy
If necessary, the procedure can be repeated 1 - 2 weeks later. Corticosteroids may also be injected into the tympanic cavity after aspiration.
If the effusion is too viscous to be aspirated via tympanocentesis, a myringotomy is performed.
Under local anesthesia (general anesthesia for children), a radial or curved incision is placed in the anteroinferior quadrant of the tympanic membrane using a myringotomy knife. Care is taken to avoid damaging the mucosa of the middle ear cavity, and all effusion is suctioned out.
For patients with persistent or recurrent disease, or for cases with highly viscous effusion that is difficult to drain, tympanostomy tube insertion may be considered to improve ventilation and drainage and promote recovery of Eustachian tube function.
Eustachian tube balloon dilation may also be considered to restore Eustachian tube function.
For cases with chronic recurrence, CT values exceeding 40 HU, or suspected granulation tissue in the middle ear or mastoid cavity, exploratory surgery may be performed as needed.
For recurrent or severe tonsillitis, or hypertrophic tonsils associated with recurrent secretory otitis media, tonsillectomy should be performed.
Complications
Some cases of secretory otitis media may progress to the following conditions:
- Adhesive otitis media
- Tympanosclerosis
- Cholesterol granuloma
- Acquired primary cholesteatoma of the middle ear