Paroxysmal supraventricular tachycardia (PSVT) is the most common ectopic rapid arrhythmia in children. It refers to tachycardia caused by ectopic excitation originating above the bundle of His, primarily due to reentry mechanisms, with a smaller proportion caused by enhanced automaticity or triggered activity. This condition can occur at any age, is prone to recurrent episodes, and is most commonly seen for the first time during infancy.
Etiology
PSVT can occur in the context of congenital heart disease, Wolff-Parkinson-White syndrome, myocarditis, or endocardial fibroelastosis. However, most affected children do not have organic heart disease. Infections represent a common trigger, but other precipitating factors may include fatigue, emotional stress, hyperventilation, cardiac surgery (perioperative period), and cardiac catheterization.
Clinical Manifestations
Children with this condition often experience an abrupt onset of irritability, pallor or cyanosis, cold and clammy skin, rapid breathing, and a weak pulse, often accompanied by a dry cough and, occasionally, vomiting. Older children may report palpitations, discomfort in the precordial region, dizziness, and other symptoms. During an episode, the heart rate typically increases suddenly, ranging from 160 to 300 beats per minute, and the duration of each episode may vary from several seconds to several days. Upon termination of the episode, the heart rate abruptly slows down and returns to normal. Key features of PSVT include regular and fixed heart rates during episodes, as well as heart sounds with uniformly strong first heart tones during auscultation. If an episode lasts longer than 24 hours, there is a risk of developing heart failure.
Diagnosis
Electrocardiographic features include abnormal P waves that are often smaller than normal and may overlap with the preceding T wave, rendering them indistinguishable. The QRS complex morphology is similar to that seen in sinus tachycardia. Prolonged episodes may lead to transient changes in the ST segment and T wave. Some children may show signs of Wolff-Parkinson-White syndrome during the interictal period. Differential diagnosis may be required to distinguish PSVT from sinus tachycardia and ventricular tachycardia.
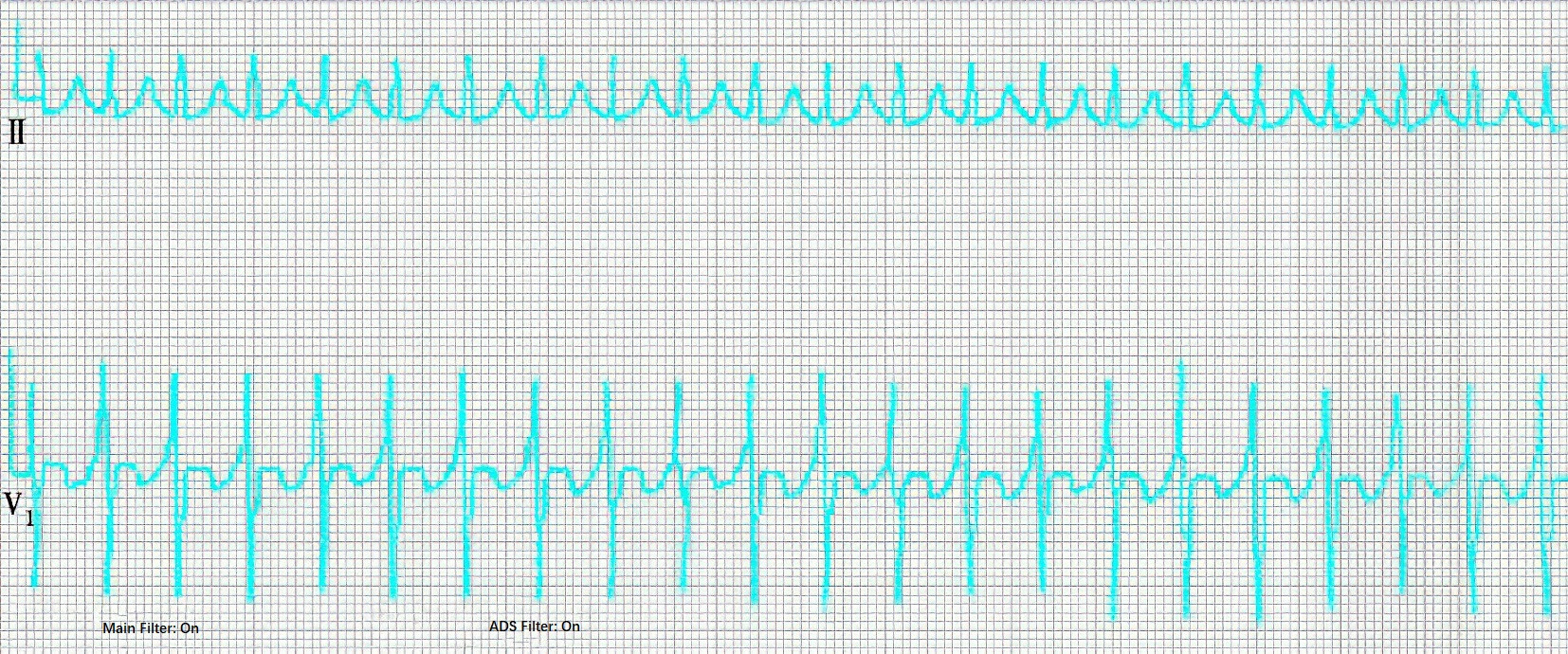
Figure 1 Electrocardiographic features of paroxysmal supraventricular tachycardia
Treatment
Stimulation of the Vagus Nerve to Terminate Episodes
Children without structural heart disease or significant heart failure may benefit from vagal maneuvers, such as pharyngeal stimulation using a tongue depressor or finger to induce gagging or vomiting, or encouraging the child to take a deep breath and hold it. If ineffective, carotid sinus pressure or the diving reflex method may be attempted.
Pharmacological Treatment
Medication may be considered if the above methods prove ineffective or are effective only transiently with rapid relapse. The following options are used depending on the clinical scenario:
Digitalis Drugs
These are indicated for more severe cases, particularly when episodes last over 24 hours and heart failure symptoms are present. Contraindications include ventricular tachycardia or PSVT caused by digitalis toxicity. Caution is required in cases of hypokalemia, myocarditis, PSVT with AV conduction block, or impaired renal function.
Beta-Blockers
These are contraindicated in patients with severe AV block, asthma, or heart failure.
Selective Calcium Channel Blockers
These drugs inhibit calcium ion entry into cells and have demonstrated efficacy. Side effects include hypotension and negative inotropic effects, which may exacerbate AV block. They are contraindicated for infants under one year of age.
Sodium Channel Blockers
These can effectively terminate PSVT and are associated with fewer side effects.
Electrical Therapy
For patients who do not respond well to medications, particularly those with hemodynamic instability (excluding cases of digitalis toxicity), synchronized direct current cardioversion may be used. Alternative techniques, where available, include transesophageal atrial pacing or intracardiac pacing via the right atrium, which can terminate PSVT episodes.
Radiofrequency Ablation (RFA)
This method may be considered for cases where medications are ineffective, episodes occur frequently, or episodes are prolonged and accompanied by cardiac dysfunction.
Prognosis
Most patients respond well to medical treatment. If prolonged episodes are left untreated, they may result in heart failure and negatively affect the prognosis.