Shoulder dystocia refers to the condition where, after the fetal head has been delivered, the anterior shoulder becomes impacted behind the pubic symphysis, and standard obstetric maneuvers are ineffective in delivering the fetal shoulders. Defining shoulder dystocia based on the time interval between the delivery of the head and body lacks sufficient evidence. Its incidence varies depending on fetal weight: 0.3%–1% for fetuses weighing 2,500 to <4,000 g; 3%–12% for 4,000 to <4,500 g; and 8.4%–14.6% for ≥4,500 g. More than half of shoulder dystocia cases occur in newborns with normal birth weight, making accurate prediction and prevention difficult.
Risk Factors
Prenatal risk factors include:
- Fetal macrosomia
- History of shoulder dystocia
- Gestational hyperglycemia
- Post-term pregnancy
- Abnormal pelvic anatomy
Intrapartum risk factors include:
- Prolonged active phase of the first stage of labor
- Prolonged second stage accompanied by the “turtle sign” (retraction of the fetal head after delivery)
- Use of vacuum or forceps for assisted delivery
Maternal and Neonatal Impact
Maternal Complications
Severe perineal lacerations (third- and fourth-degree) and postpartum hemorrhage may occur.
Additional complications may include cervical laceration, uterine rupture, genital tract fistulas, and puerperal infections
Neonatal Complications
Brachial plexus injury is the most common, with two-thirds of cases involving Duchenne-Erb palsy, resulting from damage to the C5–C6 nerve roots; most are temporary.
The asymmetrical force exerted by the maternal expulsive efforts, in addition to assisted delivery maneuvers, can contribute to nerve injury.
Other complications may include clavicular fracture, humeral fracture, neonatal asphyxia, and in severe cases, intracranial hemorrhage, neurological impairment, or neonatal death.
Diagnosis
Shoulder dystocia can be diagnosed when, after delivery of the fetal head, the head retracts, the fetal chin presses tightly against the perineum, and the shoulders cannot be delivered. Fetal abnormalities should be ruled out.
Management
Reducing the interval between head and body delivery is critical for neonatal survival. Preparations for neonatal resuscitation should be in place.
Calling for Assistance and Performing Episiotomy
Once shoulder dystocia is diagnosed, experienced obstetricians, anesthesiologists, midwives, and pediatricians should be called to assist. Episiotomy or extension of the incision should be performed to increase vaginal space for maneuvers.
McRoberts Maneuver
The mother's legs should be hyperflexed and brought close to the abdomen, with hands holding the knees. This maneuver reduces pelvic tilt, straightens the lumbosacral curve, and causes the sacrum to shift posteriorly and the sacroiliac joint to widen slightly. These changes help dislodge the anterior shoulder from behind the pubic symphysis. Gentle downward traction on the fetal head may assist in delivery of the shoulder.
Suprapubic Pressure
The provider locates the fetal anterior shoulder above the pubic symphysis and applies pressure downward and posteriorly. This may reduce the bisacromial diameter, while gentle traction on the fetal head is applied. Forceful pulling must be avoided. Over 50% of shoulder dystocia cases can be resolved using the McRoberts maneuver with suprapubic pressure.
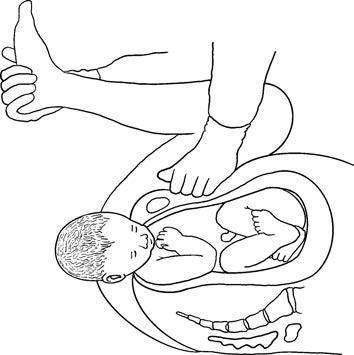
Figure 1 McRoberts maneuver with suprapubic pressure
Delivery of the Posterior Arm
The provider inserts a hand along the sacrum to reach the fetal posterior arm, flexes the elbow across the fetal chest, and delivers the arm using a “reverse face-washing” motion. Grasping the upper arm should be avoided to prevent humeral fracture. This method successfully resolves over 95% of cases within 4 minutes.
Rotational Maneuvers (Rubin and Woods Techniques)
Rubin Maneuver
The provider inserts fingers behind the fetal anterior shoulder, pushing the scapula toward the fetal chest to rotate the shoulders into the oblique diameter of the pelvis and release the impacted anterior shoulder
Woods Maneuver
The provider inserts fingers in front of the posterior shoulder, applying pressure in the direction of the fetal back to rotate the posterior shoulder toward the pubic symphysis
These two methods may be combined to assist shoulder rotation and delivery
Gaskin Maneuver (All-Fours Position)
The mother is assisted into a hands-and-knees position. The gravitational shift and potential changes in pelvic dimensions may help dislodge the impacted shoulder. This position can be considered in conjunction with the aforementioned techniques.
If these methods fail, more invasive procedures may be necessary, including:
- Zavanelli maneuver (replacement of the fetal head followed by cesarean delivery)
- Symphysiotomy
- Clavicular fracture (cleidotomy)
These interventions carry significant risks and must be performed with strict indications and caution.