HELLP syndrome (hemolysis, elevated liver enzymes, and low platelet count syndrome) is characterized by hemolysis, elevated transaminase levels, and thrombocytopenia, occurring in the context of preeclampsia-eclampsia. It represents a severe manifestation of preeclampsia and is associated with significant maternal and fetal risks.
Etiology and Pathogenesis
The underlying pathological changes in HELLP syndrome are similar to those of preeclampsia, although the exact causes and mechanisms remain unclear. Autoimmune processes are thought to play a significant role.
Impact on the Mother and Fetus
Maternal Impact
Pregnant women with HELLP syndrome may experience complications such as pulmonary edema, placental abruption, ascites, postpartum hemorrhage, disseminated intravascular coagulation (DIC), renal failure, and liver rupture. Cesarean delivery rates are high, and maternal mortality is significantly elevated. Studies indicate that multiorgan failure and DIC are the leading causes of death in HELLP syndrome.
Fetal Impact
Fetal complications arise from insufficient placental blood and oxygen supply, as well as placental dysfunction. These may include fetal growth restriction, stillbirth, and preterm delivery.
Clinical Presentation
Common symptoms include upper right abdominal or epigastric pain, nausea, vomiting, and general malaise, which are nonspecific. Mild jaundice may be present in some cases. Physical examination may reveal muscle rigidity in the upper right abdominal or epigastric region, sudden weight gain, and edema. Severe coagulation abnormalities can lead to hematuria and gastrointestinal bleeding.
HELLP syndrome can occur at any time from mid-pregnancy to several days postpartum, with over 70% of cases occurring before delivery.
Diagnosis
The diagnosis of HELLP syndrome relies heavily on laboratory findings due to its nonspecific clinical presentation. Diagnostic criteria include the following:
Intravascular Hemolysis
Abnormal red blood cell findings such as schistocytes and spherocytes in a peripheral blood smear. Serum total bilirubin ≥20.5 μmol/L and serum haptoglobin <250 mg/L.
Elevated Liver Enzymes
Serum transaminase levels exceeding twice the normal upper limit. Elevated lactate dehydrogenase (LDH) levels, often defined as LDH ≥600 U/L.
Low Platelet Count
Platelet count <100×109/L.
Elevated LDH levels and decreased serum haptoglobin levels are considered sensitive indicators, often appearing before increases in unconjugated bilirubin and decreases in hemoglobin levels.
Differential Diagnosis
HELLP syndrome should be differentiated from other conditions, including thrombotic thrombocytopenic purpura (TTP), hemolytic uremic syndrome (HUS), and acute fatty liver of pregnancy.
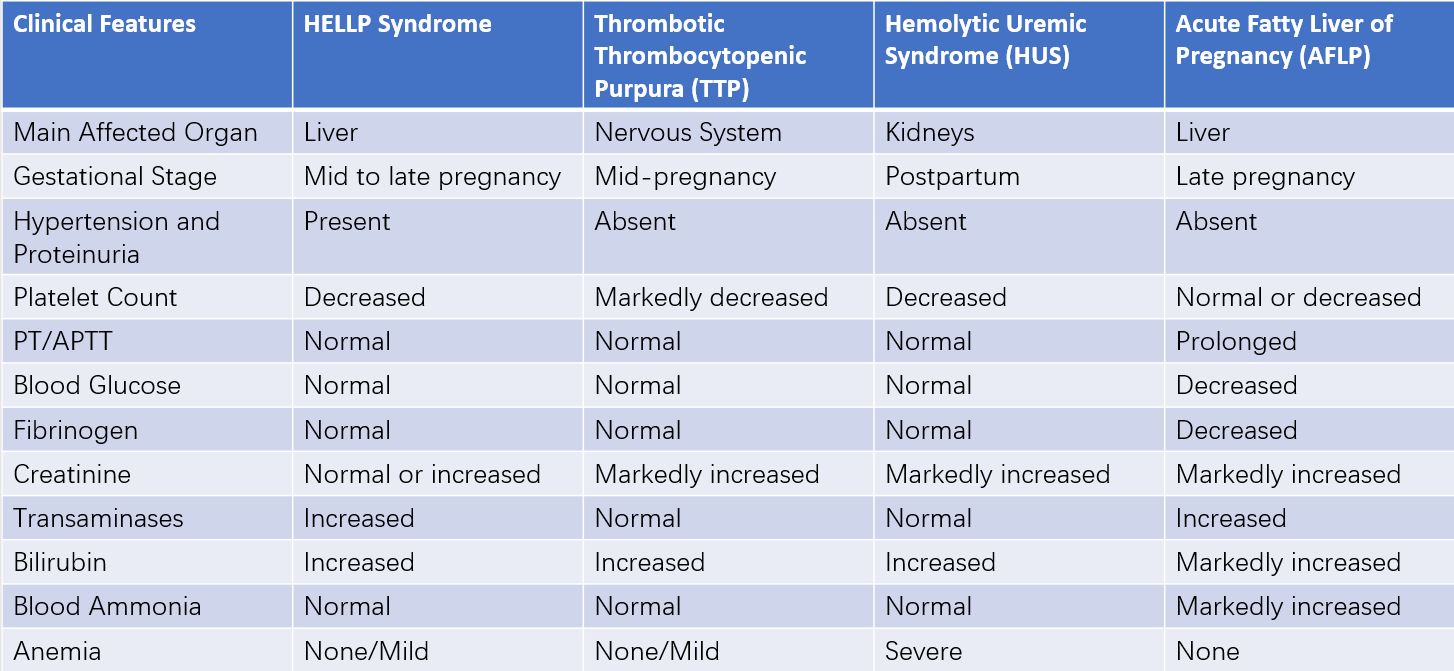
Table 1 Differential diagnosis of HELLP syndrome
Note:
PT: Prothrombin Time
APTT: Activated Partial Thromboplastin Time
Treatment
The treatment principles involve managing the condition on the basis of severe preeclampsia protocols, controlling disease progression, preventing severe complications, and terminating the pregnancy when necessary.
Blood Product Transfusion
Blood products, such as red blood cell suspensions, fresh frozen plasma, and platelet concentrates, are used when hemolysis, coagulation dysfunction, or severe thrombocytopenia occurs. Indications for platelet transfusion include:
- Platelet count <20×109/L before vaginal delivery.
- Platelet count <50×109/L before cesarean delivery.
- Significant active bleeding.
- Known platelet function disorders.
- Rapid platelet count decline.
- Coagulation dysfunction.
Corticosteroids
Dexamethasone is a commonly used corticosteroid in the management of HELLP syndrome, particularly when the platelet count is <50×10⁹/L. However, its efficacy in improving adverse pregnancy outcomes remains controversial.
Pregnancy Termination
The only definitive treatment for HELLP syndrome is termination of pregnancy.
Time to Termination
Immediate pregnancy termination is required if the gestational age is ≥34 weeks, fetal lung maturity is confirmed, fetal distress is detected, subcapsular liver hematoma is present, or maternal condition worsens. In stable cases with gestational age <34 weeks, fetal lung immaturity, and no significant fetal distress, pregnancy may be prolonged for 48 hours to complete corticosteroid therapy for fetal lung maturation before termination.
Mode of Delivery
HELLP syndrome is not an absolute indication for cesarean delivery, although indications may be relaxed based on the clinical situation.
Anesthetic Considerations
Due to thrombocytopenia and the associated risk of localized bleeding, pudendal block and epidural anesthesia are contraindicated. Local infiltration anesthesia is recommended for vaginal delivery, while local infiltration anesthesia or general anesthesia may be utilized for cesarean delivery.