Before 28 weeks of gestation, the fetus is relatively small, and the amount of amniotic fluid is relatively abundant, allowing the fetus greater mobility within the uterus. During this period, the fetal position is not fixed. After 32 weeks, rapid fetal growth and a relative decrease in amniotic fluid bring the fetus closer to the uterine wall, resulting in a relatively stable fetal attitude and position. However, in rare cases, fetal attitude and position may change during late pregnancy. Fetal position may even alter during labor. The diagnosis of fetal position requires comprehensive evaluation using abdominal palpation (Leopold’s maneuvers), vaginal or rectal examination, and ultrasound.
Fetal Attitude
The term "fetal attitude" refers to the posture of the fetus within the uterus. A normal fetal attitude is characterized by flexion of the fetal head, with the chin resting against the chest, a slightly curved spine, and flexed limbs crossed in front of the chest and abdomen. In this posture, the fetus's body volume and surface area are minimized, and the overall fetal form resembles an oval shape.
Fetal Lie
Fetal lie describes the relationship between the fetal longitudinal axis and the maternal longitudinal axis (as shown in Figure 5-2). When the fetal longitudinal axis is parallel to the maternal longitudinal axis, this is termed a longitudinal lie, which accounts for 99.75% of full-term deliveries. If the fetal longitudinal axis is perpendicular to the maternal longitudinal axis, this is referred to as a transverse lie, making up only 0.25% of full-term deliveries. A oblique lie is when the fetal longitudinal axis intersects the maternal longitudinal axis at an angle. Oblique lie is typically transient and often resolves into a longitudinal lie during labor, though occasionally it may become a transverse lie.
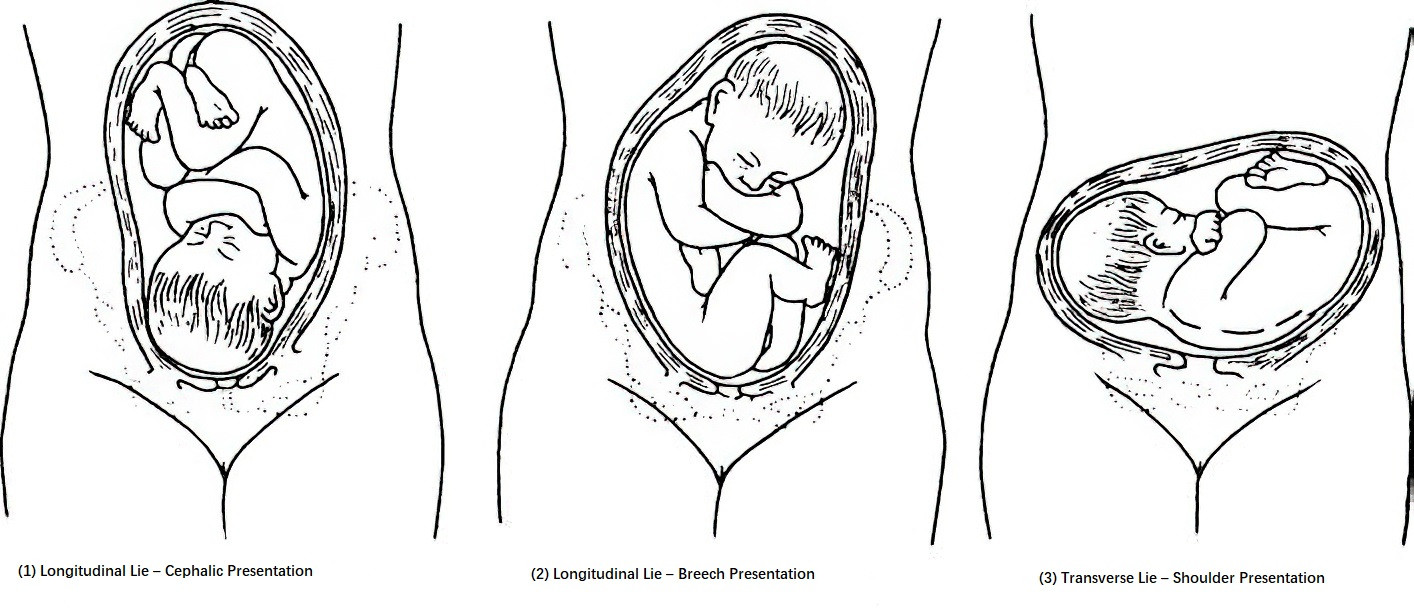
Figure 1 Types of fetal lie
Fetal Presentation
Fetal presentation describes the part of the fetus that enters the pelvic inlet first. In longitudinal lie, the presentation may be either cephalic (head-first) or breech (buttocks-first). In transverse lie, the presentation is typically the shoulder. Cephalic presentation is further classified based on the degree of flexion or extension of the fetal head, into vertex (occiput-first), sinciput (anterior fontanel), brow, or face presentations. Breech presentations are categorized as complete breech (hips and knees flexed), frank breech (hips flexed, knees extended), and footling breech, which may involve one foot (single footling) or both feet (double footling). In transverse lie, the shoulder is the presenting part, referred to as shoulder presentation. Rarely, a compound presentation occurs, in which the head or breech enters the pelvis with a fetal hand or foot simultaneously.
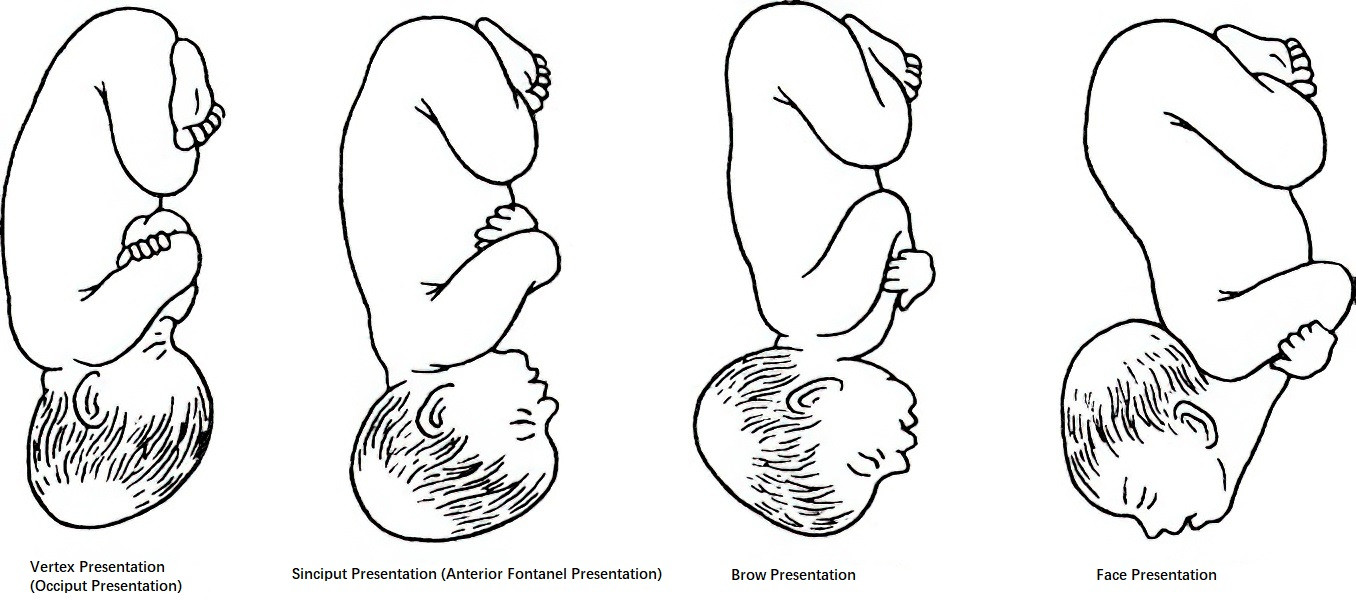
Figure 2 Types of cephalic presentation
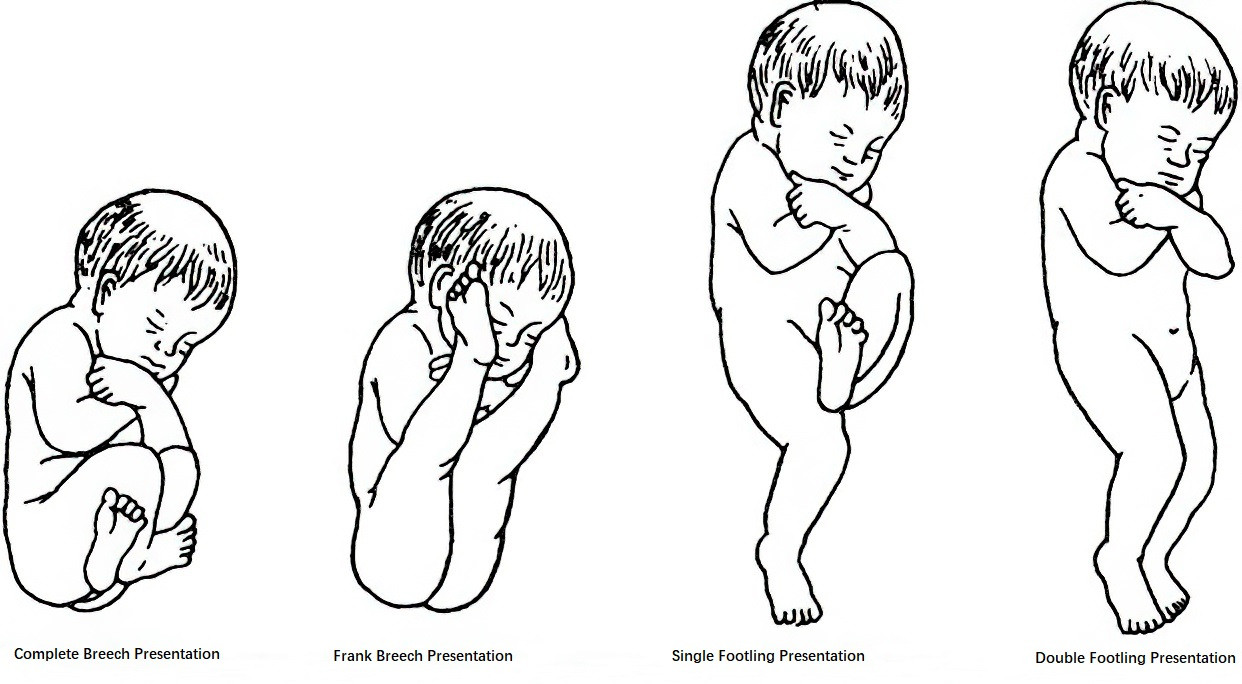
Figure 3 Types of breech presentation
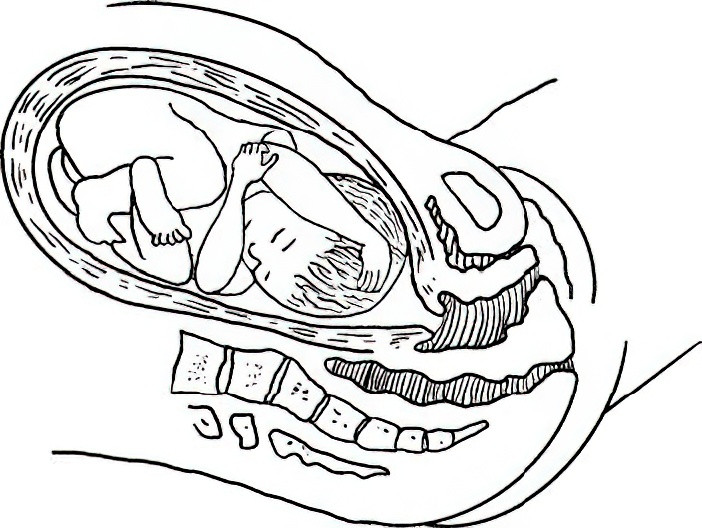
Figure 4 Compound presentation
Fetal Position
Fetal position describes the relationship between the reference point on the presenting part and the maternal pelvis. For cephalic (vertex) presentation, the reference point is the occiput; for face presentation, it is the chin; for breech presentation, it is the sacrum; and for shoulder presentation, it is the scapula. Fetal positions are classified based on the location of the reference point relative to the maternal pelvic inlet—left, right, anterior, posterior, or transverse. For cephalic, face, and breech presentations, there are six possible fetal positions, whereas shoulder presentation has four. For example, in cephalic presentation, if the occiput is located in the left anterior quadrant of the maternal pelvis, the position is termed left occiput anterior (LOA). Other positions are named accordingly.
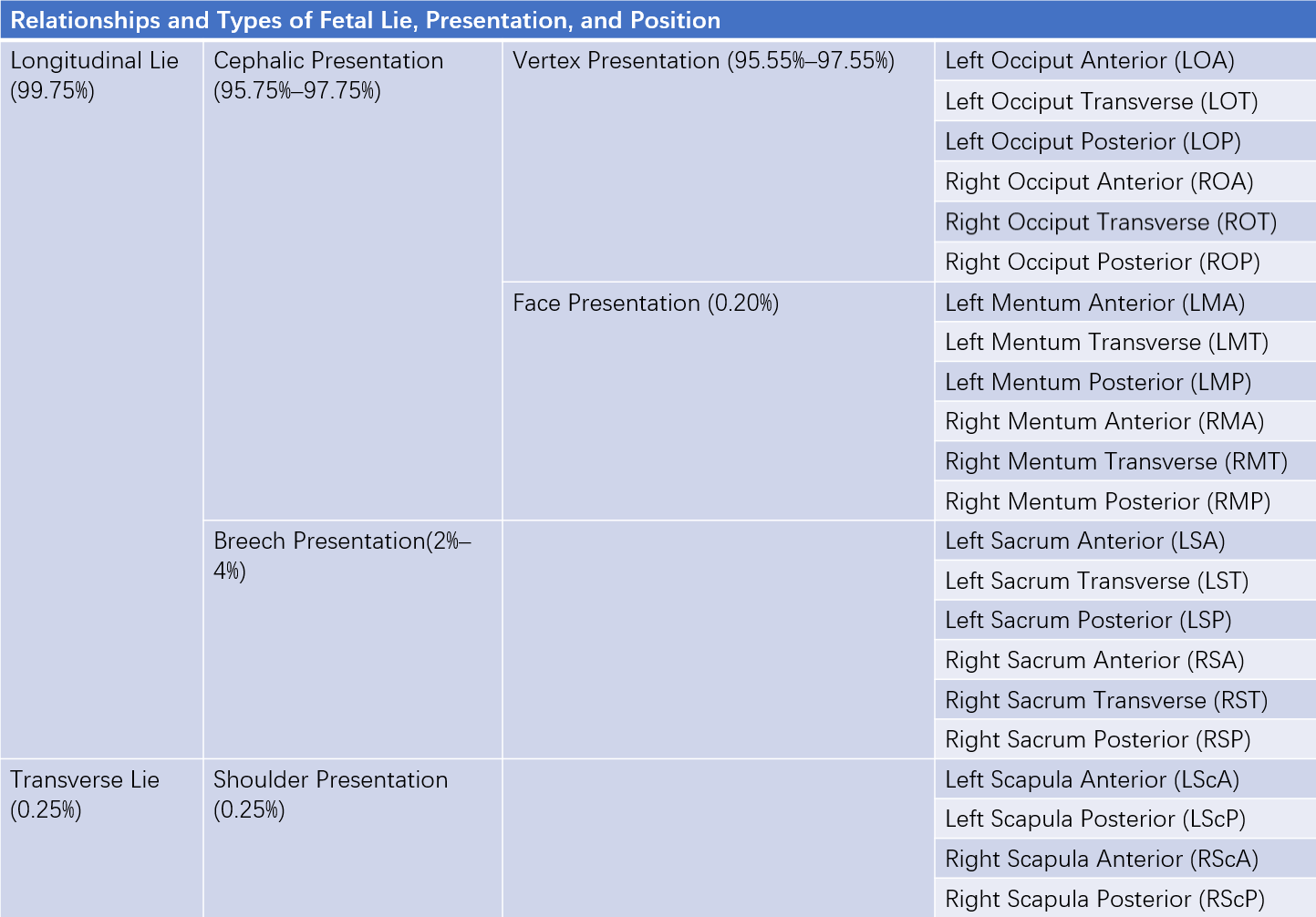
Table 1 Relationships and types of fetal lie, presentation, and position