The nose consists of the external nose, the nasal cavity, and the paranasal sinuses. The nasal cavity is an irregular space with a complex internal structure, particularly evident on its lateral walls. Each side of the nasal cavity is connected to four groups of paranasal sinuses through deep and concealed sinus openings. The paranasal sinuses have intricate anatomical relationships with structures such as the orbit, the anterior and middle cranial base (including the intracranial segment of the internal carotid artery and the cavernous sinus). These relationships form the anatomical foundation for nose-eye and nose-cranium surgeries.
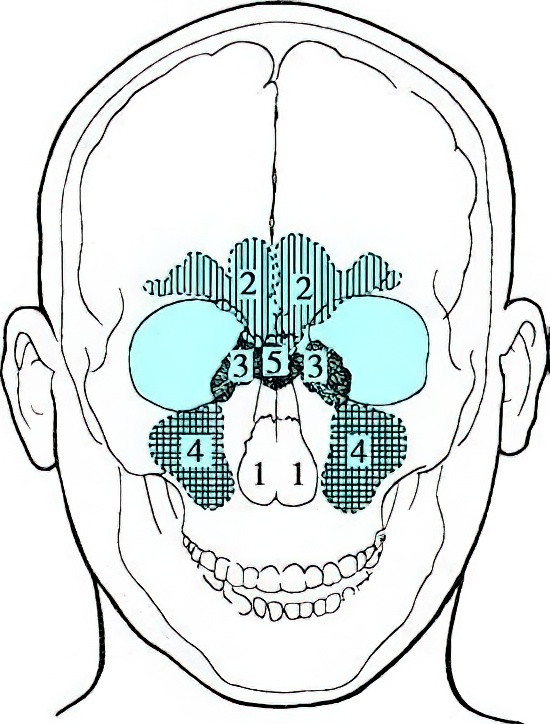
Figure 1 The Position of the nose in the craniofacial skeleton
1, Nasal cavity
2, Frontal sinus
3, Ethmoid sinus
4, Maxillary sinus
5, Sphenoid sinus
External Nose
Shape
The external nose is composed of bone and cartilage, covered by skin and soft tissue. It appears narrow at the top and wide at the bottom, taking the shape of a downward-facing triangular pyramid. The upper part of the anterior ridge is the nasal root, followed sequentially by the midline nasal bridge and the nasal apex at the lower anterior end. The sides of the nasal bridge form the nasal dorsum, while the semi-circular protrusions on either side of the nasal apex form the alae nasi. The base of the pyramid is the nasal base (basis nasi), where the lower margin of the nasal septal cartilage and the medial crura of the greater alar cartilage form the columella nasi. The nasal base extends forward into the left and right anterior nares, and the nasal wings connect externally with the cheeks along a shallow groove called the nasolabial fold.
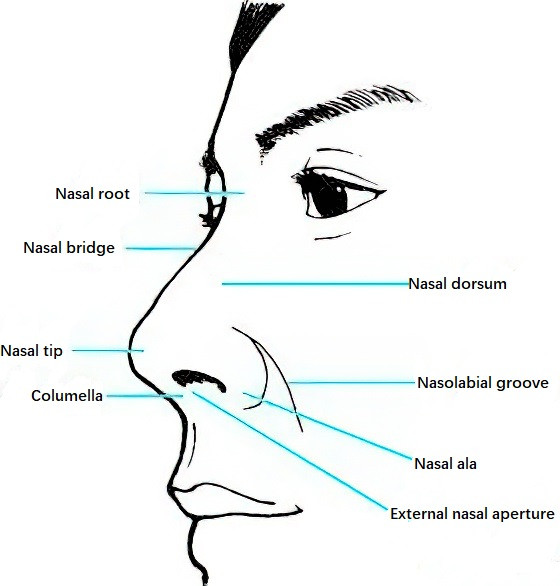
Figure 2 External nose
Cartilaginous Framework of the External Nose
The cartilaginous framework of the external nose primarily consists of the paired lateral nasal cartilage and greater alar cartilage. The lateral nasal cartilages, also known as the septodorsal cartilage or dorsal nasal plate, are bilateral triangular structures. The upper edges are connected to the lower border of the nasal bone and the frontal process of the maxilla, while the medial edges converge at the midline to connect to the anterior-superior edge of the nasal septum. The septodorsal cartilage appears inverted V-shaped in a bottom view, with its lateral wings forming the lateral nasal cartilage (dorsal nasal plate) and the central part forming the septal nasal plate. The greater alar cartilage, also known as the lower lateral nasal cartilage, is horseshoe-shaped. Its lateral crura provide structural support to the alae nasi, while the medial crura join the anterior-inferior edge of the nasal septal cartilage to form the columella framework. Additional accessory nasal cartilages (small alar cartilages and sesamoid cartilages) fill the space between the lateral nasal cartilage and the greater alar cartilage.
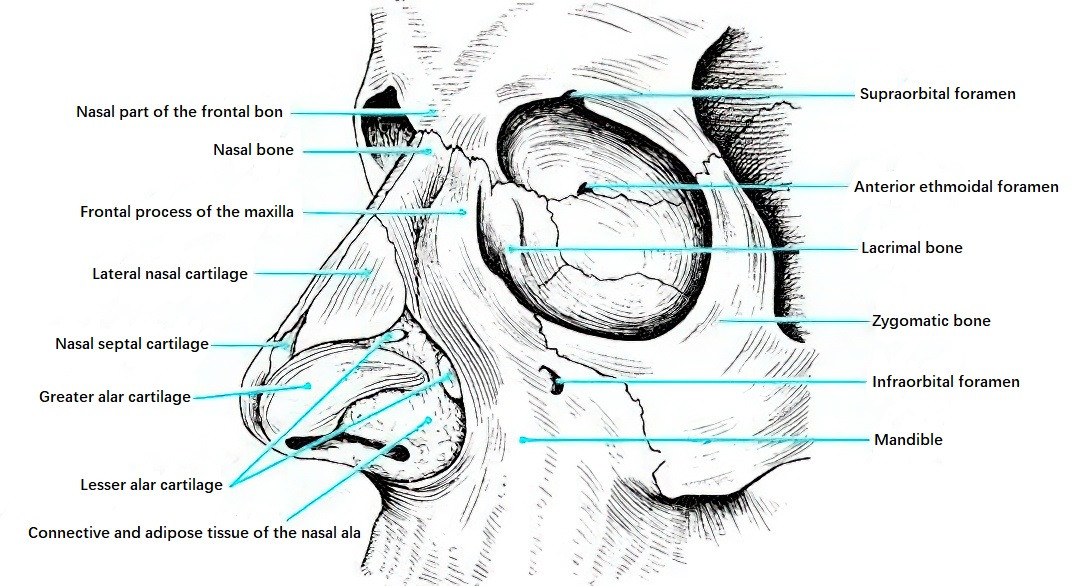
Figure 3 Bony and cartilaginous framework of the external nose
Bony Framework of the External Nose
The bony framework of the external nose is formed by the nasal bones, the nasal process of the frontal bone, and the frontal process of the maxilla. The paired nasal bones connect superiorly to the frontal bone, laterally to the frontal process of the maxilla, and inferiorly to the upper edge of the lateral nasal cartilage. Posteriorly, the nasal bones have a nasal crest, which connects to the frontal crest, the vertical plate of the ethmoid bone, and the nasal septal cartilage. The upper part of the nasal bone is narrow and thick with good protective functions, while the lower part is wide and thin, making it prone to fractures. The lower edge of the nasal bones, the inner edge of the maxilla's frontal process, and the free edge of the maxilla's palatine process together form the pyriform aperture.
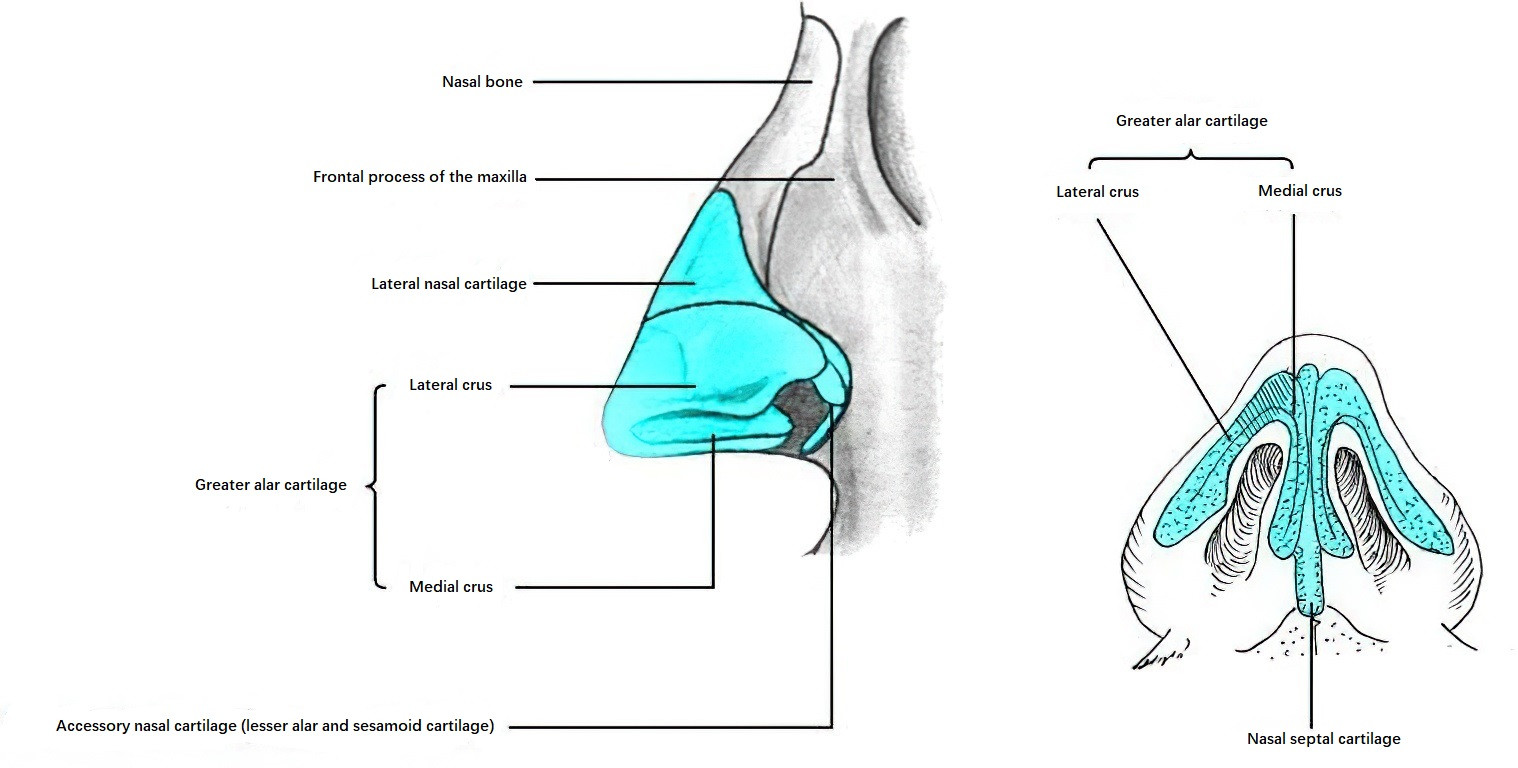
Figure 4 Cartilaginous framework of the external nose (Lateral and inferior views)
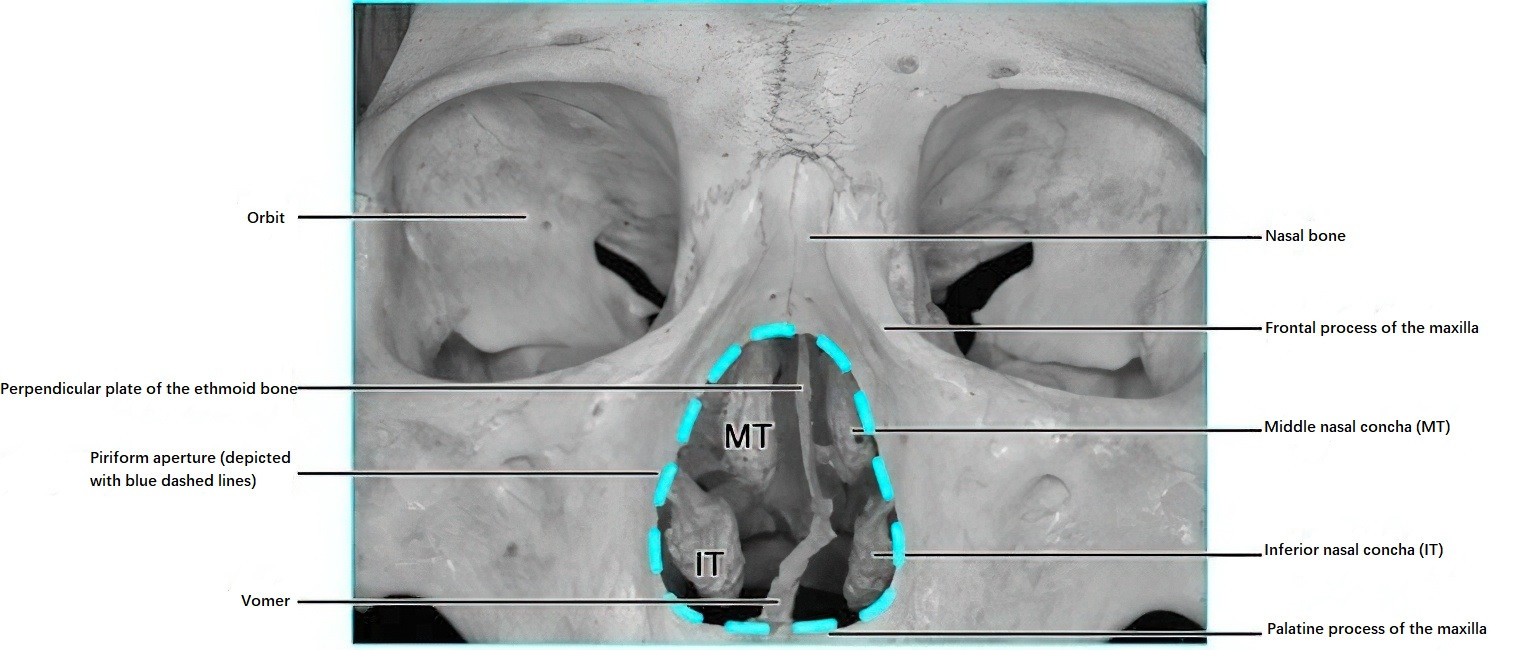
Figure 5 Nasal aperture (Piriform aperture)
Skin of the External Nose
The skin of the nasal tip, alae nasi, and nasal vestibule is relatively thick and is closely connected to the underlying fatty-fibrous tissue and perichondrium. This close attachment makes nerve endings more susceptible to pressure during inflammation, leading to pronounced pain with minimal swelling. The skin of the nasal tip and alae nasi contains a higher density of sweat glands and sebaceous glands, making it prone to acne, furuncles, or rosacea.
Venous Drainage of the External Nose
The veins of the external nose primarily drain into the angular vein and facial vein (also known as the anterior facial vein, vena facialis anterior) and subsequently into the internal jugular vein. However, the angular vein may also communicate with the cavernous sinus via the superior and inferior ophthalmic veins.
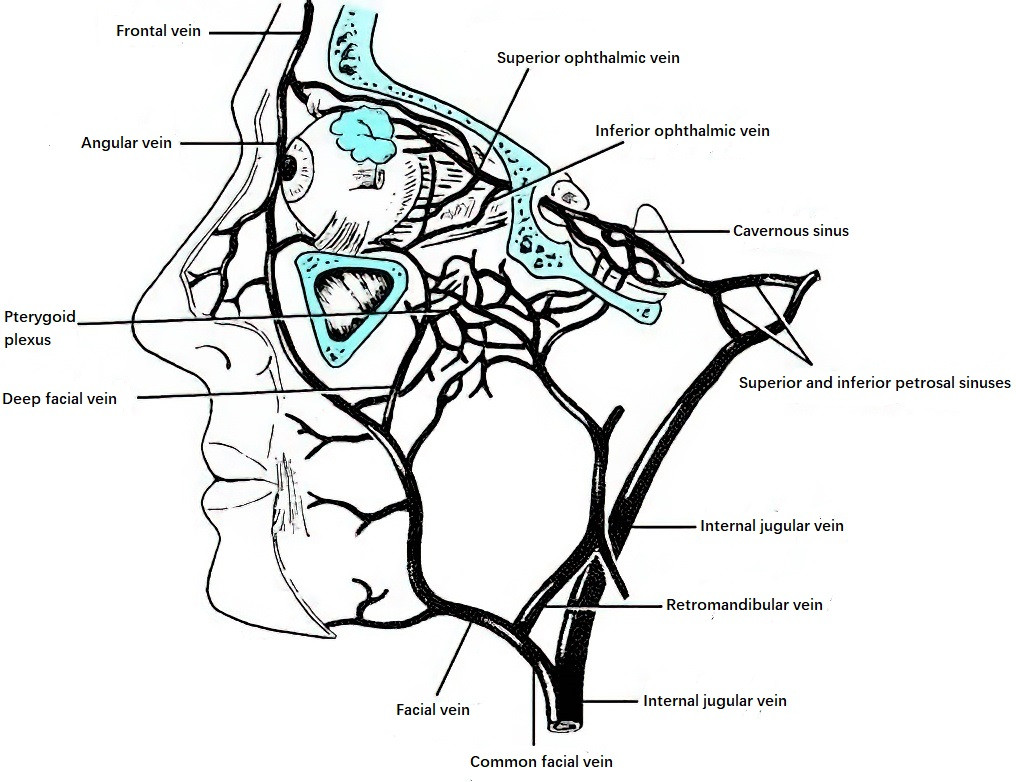
Figure 6 Venous system of the external nose and its relationship to the orbital veins and cavernous sinus
Due to the absence of valves in the facial veins, bidirectional blood flow is possible. This predisposes infections of nasal skin, such as furuncles, to complications like cavernous sinus thrombophlebitis, which can be life-threatening. Clinically, the triangular region formed by the nasal root and upper lip is referred to as the "danger triangle."
Innervation of the External Nose
Motor innervation is provided by the buccal branch of the facial nerve, which governs movement of the nasal region.
Sensory innervation is primarily provided by the ophthalmic and maxillary branches of the trigeminal nerve. The ophthalmic nerve exits from the semilunar ganglion of the trigeminal nerve and enters the orbit through the superior orbital fissure. It divides into three main branches: the frontal nerve, the lacrimal nerve, and the nasociliary nerve.
- The anterior ethmoidal nerve, a branch of the nasociliary nerve, has an external nasal branch that supplies the nasal tip.
- The supratrochlear nerve, a branch of the frontal nerve, innervates the nasal root.
- The infratrochlear nerve, a branch of the nasociliary nerve, also innervates the nasal root.
- The infraorbital nerve, a branch of the maxillary nerve, is accompanied by the infraorbital artery and exits through the infraorbital foramen to supply the nasal alae and nasal vestibule.
Lymphatic Drainage
The lymphatic drainage of the external nose primarily flows into the submandibular lymph nodes, preauricular lymph nodes, and parotid lymph nodes.
Nasal Cavity
The nasal cavity is divided into left and right sides, each shaped like a triangle in coronal section, with a narrow apex and a wider base. The anterior nares connect to the external nose, while the posterior nares lead to the nasopharynx. The nasal septum separates the left and right sides of the cavity, and the internal opening of the nose further divides each side into the nasal vestibule and the nasal proper.
Nasal Vestibule
The nasal vestibule is bounded anteriorly by the anterior nares and posteriorly by the internal opening, marked by a curved elevation on the inner side of the nasal wing, referred to as the nasal limen (limen nasi). The nasal vestibule is the narrowest part of the nasal cavity. It is covered by skin, characterized by the presence of nasal hairs, sebaceous glands, and sweat glands, making it prone to conditions such as furuncles. Due to the tight connection between the skin and cartilage, furuncles in this region can cause significant pain.
Nasal Proper (Nasal Fossa Proper)
The nasal proper, also called the nasal cavity, extends from the internal opening anteriorly to the posterior nares posteriorly. It is connected to the nasal vestibule through the internal opening. The nasal proper has four walls: the roof, floor, medial wall, and lateral wall.
Roof
The roof is dome-shaped and can be divided into three sections:
- Anterior Section: Slants upwards and is formed by the nasal bone and the nasal process of the frontal bone.
- Posterior Section: Slants downwards and is formed by the anterior wall of the sphenoid sinus.
- Middle Section: Lies horizontally and is formed by the horizontal plate of the ethmoid bone, also known as the cribriform plate, which separates the nasal cavity from the anterior cranial fossa. The cribriform plate contains multiple perforations (cribriform foramina) that allow olfactory fibers to pass into the cranial cavity. It is thin and fragile, making it vulnerable to damage during trauma or surgical procedures, potentially leading to traumatic or iatrogenic cerebrospinal fluid rhinorrhea.
Floor
The floor is formed by the nasal surface of the hard palate, which separates it from the oral cavity. The anterior three-quarters are formed by the palatine process of the maxilla, while the posterior one-quarter is formed by the horizontal plate of the palatine bone.
Medial Wall
The medial wall is the nasal septum. It is composed of the septal cartilage, the perpendicular plate of the ethmoid bone, the vomer bone, and the palatine process of the maxilla. Uneven tension curves during growth, as well as genetic factors, may lead to nasal septum deviation at junctions such as between the columellar cartilage and quadrilateral cartilage at the front, or between the quadrilateral cartilage and the ethmoid perpendicular plate posteriorly, as well as at its junction with the vomer and the palatine process of the maxilla in its posteroinferior part. The nasal septum is covered by mucous membrane, which includes an outer perichondrium and periosteum.
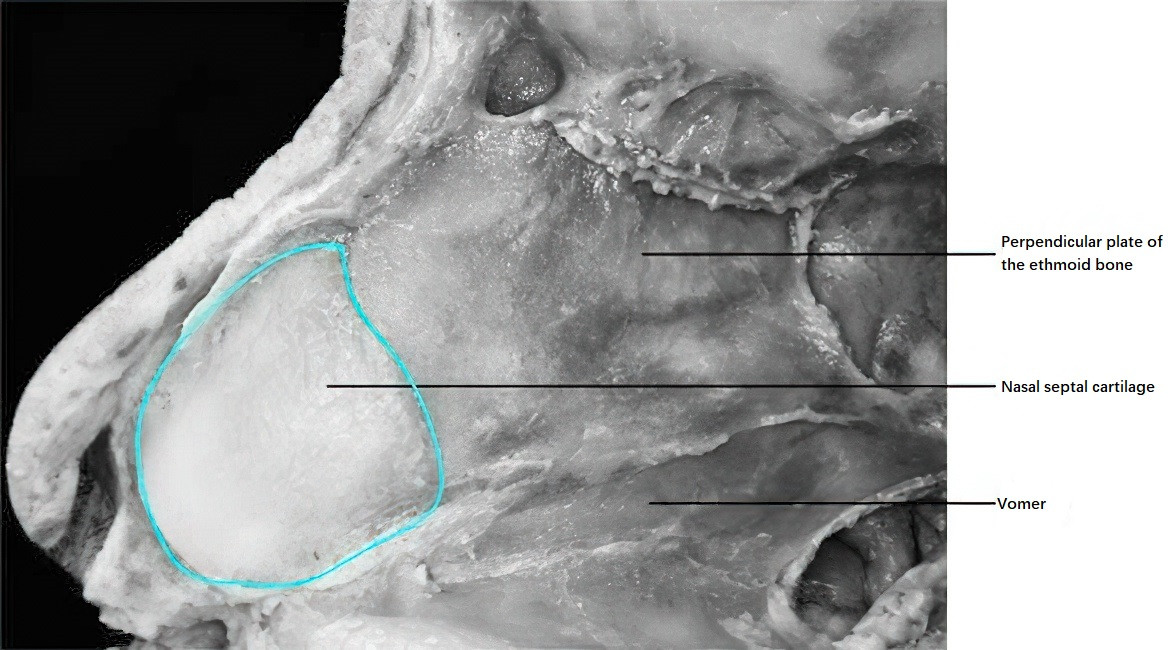
Figure 7 Nasal septal framework
Posterior Nares (Choanae)
The posterior nares are framed by the body of the sphenoid bone (roof), the medial plate of the pterygoid process of the sphenoid (lateral), the posterior edge of the horizontal plate of the palatine bone (floor), and the posterior edge of the vomer (medial). The bilateral choanae connect the nasal cavities to the nasopharynx.
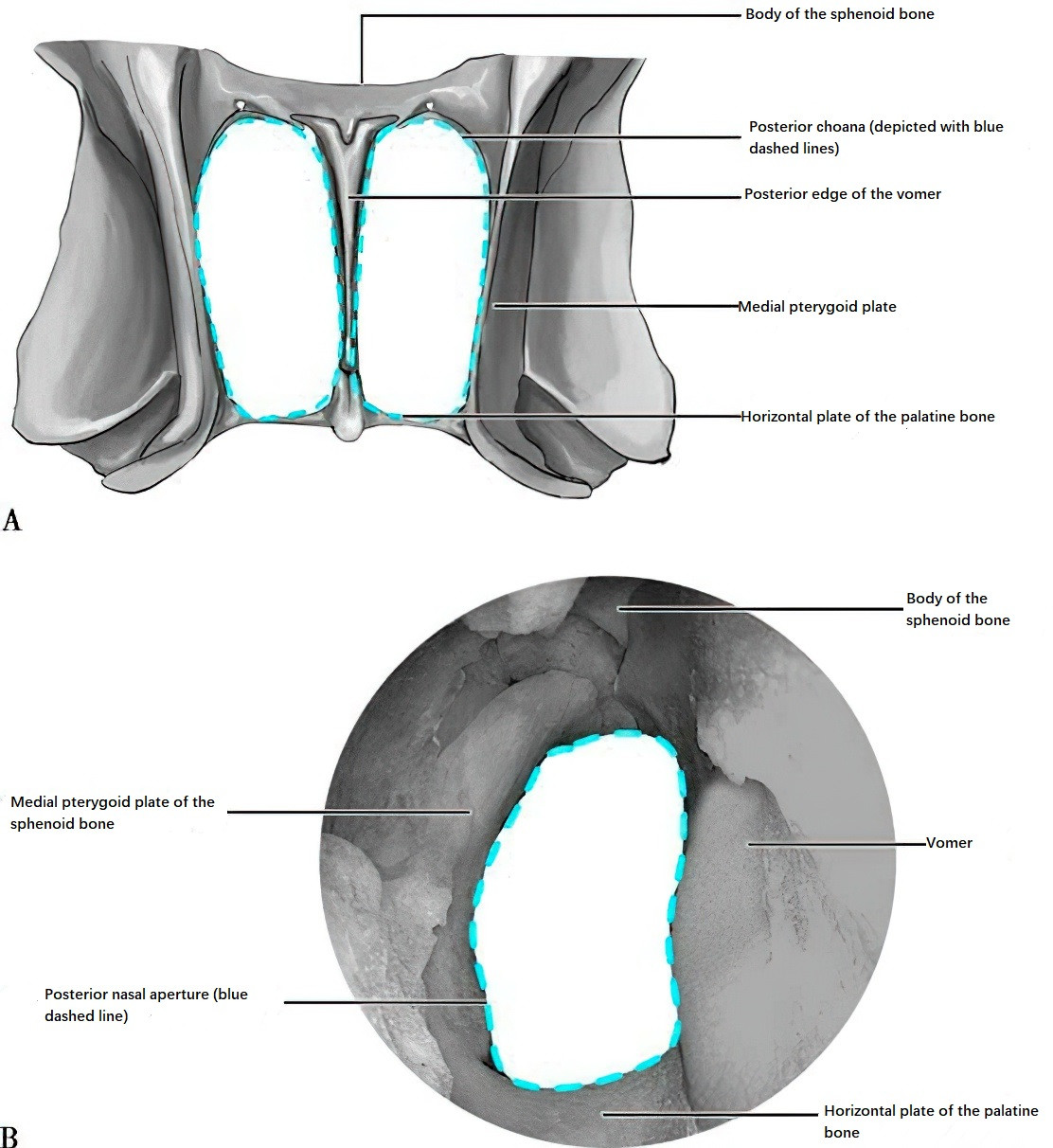
Figure 8 Bony nasal choanae
A: Schematic diagram; B: Endoscopic view of the right nasal choana.
Lateral Wall
The lateral wall is formed by the maxilla, lacrimal bone, nasal conchae, ethmoid bone (medial wall), vertical plate of the palatine bone, and the pterygoid process of the sphenoid bone. Three long, horizontally-arranged bony projections—the inferior, middle, and superior nasal conchae—extend in a steplike manner, decreasing in size by roughly one-third from bottom to top. Their anterior ends are positioned progressively further back. Below each concha, a slit-like space is formed, known as the inferior, middle, and superior meatus, respectively.
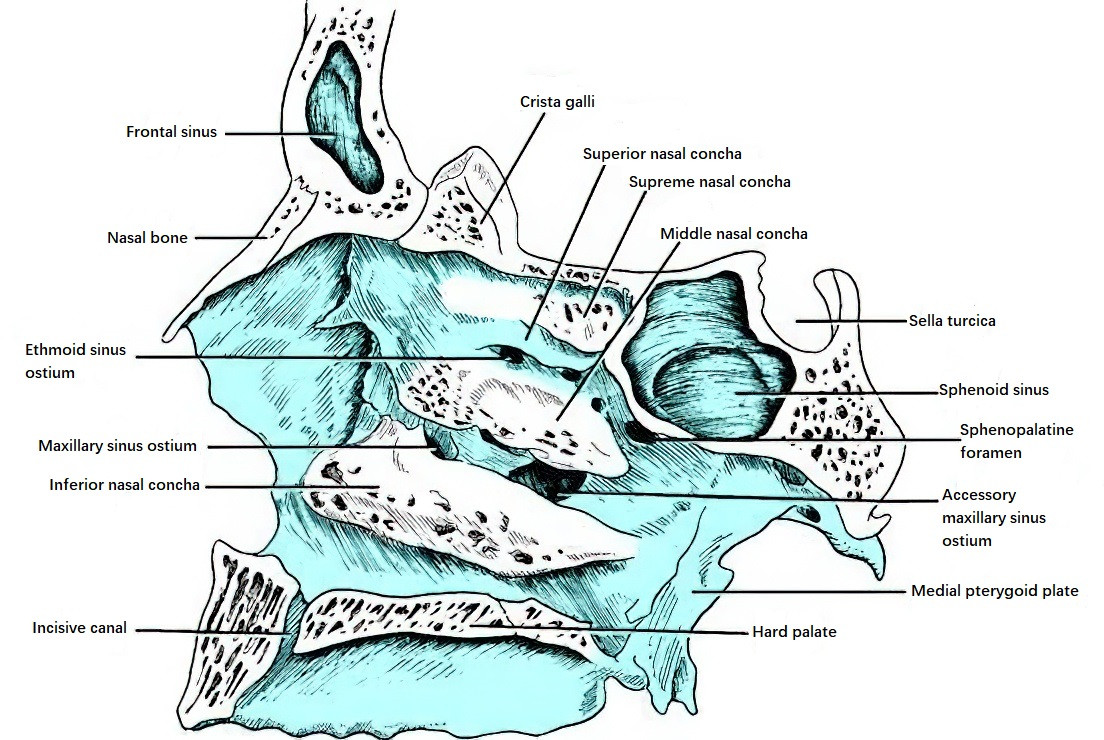
Figure 9 Structures of the bony lateral wall of the nasal cavity
Inferior Nasal Concha and Inferior Meatus
The inferior nasal concha, an independent and horizontally curved thin bone, is attached to the medial wall of the maxilla and the vertical plate of the palatine bone.
- The tear crest of its upper edge connects with the lacrimal bone, forming the nasolacrimal duct along with a bony groove at the back of the frontal process of the maxilla.
- The posterior end of the superior edge of the inferior nasal concha connects with the uncinate process of the middle nasal meatus, contributing to the formation of the natural ostium of the maxillary sinus and the nasal fontanelle.
- The lateral surface forms the inferior meatus together with the lateral wall of the nasal cavity and the attachment point of the inferior nasal concha.
The posterior end of the inferior nasal concha is approximately 1.0–1.5 cm from the pharyngeal opening of the Eustachian tube, and pathological conditions such as hypertrophy or swelling of the inferior nasal concha may directly impact the function of the Eustachian tube. The roof of the inferior meatus is dome-shaped, with the opening of the nasolacrimal duct located at its apex, roughly 3.0–3.5 cm from the anterior nares. This anatomical structure is sensitive during surgical procedures and requires cautious handling.
Middle Nasal Concha and Middle Meatus
The middle nasal concha is a critical structure of the lateral nasal wall and part of the ethmoid bone. It includes two sections:
- Anterior Section: Comprises its vertical part, which is attached to the junction of the roof of the ethmoid sinus and the horizontal plate of the ethmoid bone within the anterior cranial fossa.
- Posterior Section: Extends infero-posteriorly and changes its orientation, attaching laterally to the posterior-lower part of the lateral nasal wall (lamina papyracea). This portion of the middle nasal concha has an oblique orientation and is referred to as the lamella of the middle nasal concha. Its posterior end attaches inferiorly to the vertical process of the palatine bone and to the ethmoid crest, just anterior to the sphenopalatine foramen.
The lamella of the middle nasal concha divides the ethmoid sinuses into an anterior and posterior group.
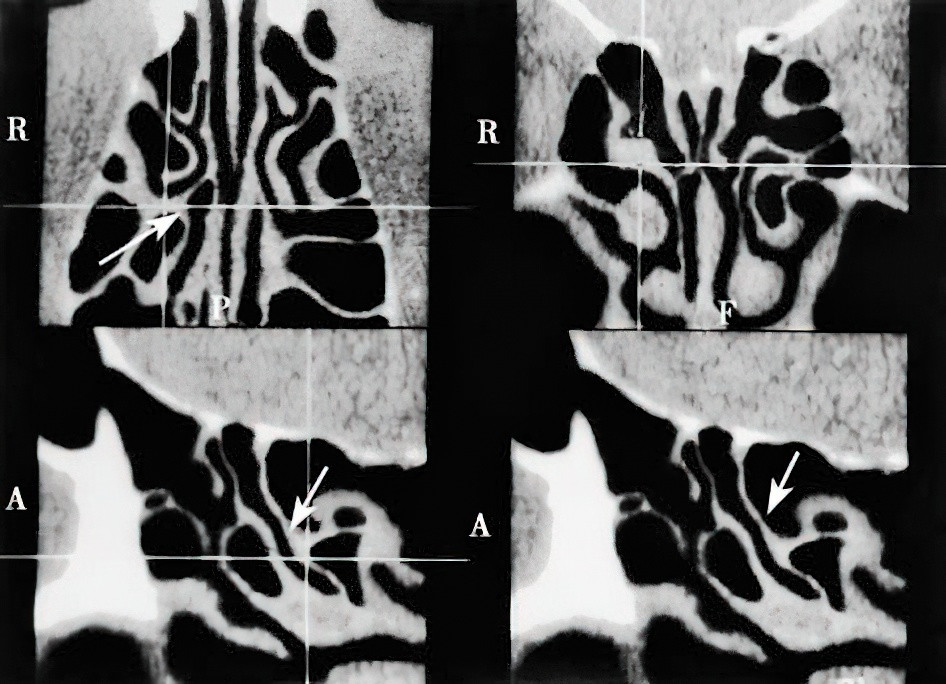
Figure 10 Axial, coronal, and sagittal CT of the nasal cavity and sinuses, highlighting the basal lamella of the middle nasal concha (Arrow)
The middle turbinate serves as an important surgical landmark. Common variations of the middle turbinate include pneumatization of the turbinate and paradoxical curvature of the turbinate (paradoxical middle turbinate). At the posterior attachment of the middle turbinate’s posterior end, approximately 12 mm superiorly and posteriorly from the upper border of the posterior nares, is the location of the sphenopalatine foramen, through which vessels and nerves pass. The space between the middle turbinate and the nasal septum above the free lower edge of the anterior middle turbinate is referred to as the olfactory sulcus or olfactory cleft. Below this level, the irregular cavity between the turbinate and the nasal septum is referred to as the common meatus.
The anatomy of the middle meatus is complex, as it contains the openings of the anterior group of paranasal sinuses. On the lateral wall of the middle meatus, there are two prominences. The anterior-inferior, crescent-shaped ridge is known as the uncinate process. Posterior to this, a rounded elevation known as the ethmoid bulla can be found, which is one of the larger air cells of the ethmoid sinus. Between these two structures lies a crescent-shaped fissure called the semilunar hiatus.
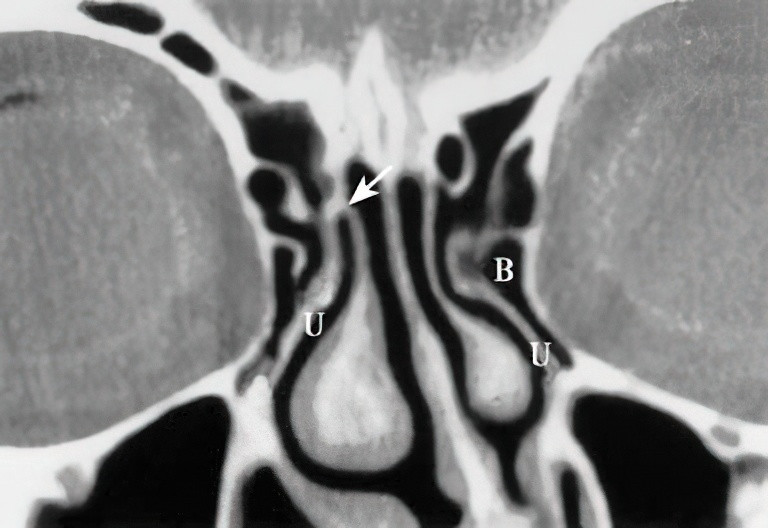
Figure 11 Coronal CT of the sinuses
This displays the uncinate process (U); the differing attachment patterns on both sides (right side attached to the skull base, left side attached to the lamina papyracea); B: Bulla ethmoidalis.
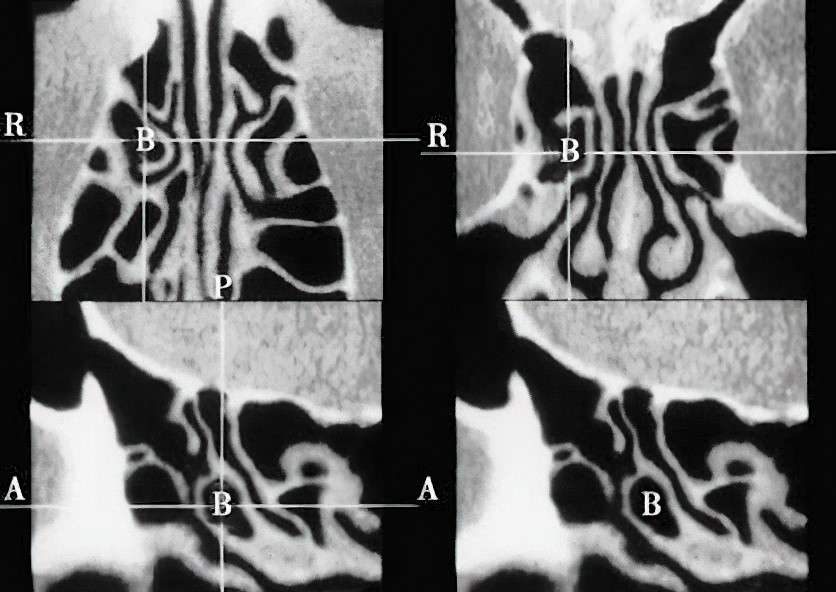
Figure 12 Axial, coronal, and sagittal CT of the sinuses, highlighting the bulla ethmoidalis (B)
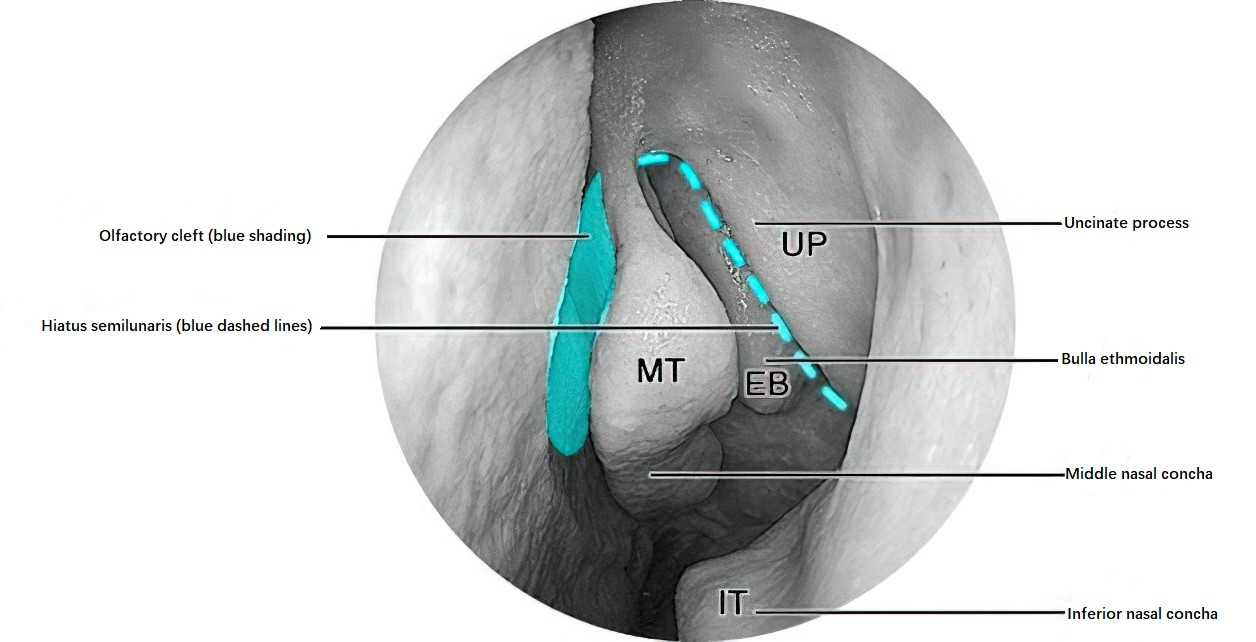
Figure 13 Endoscopic view of the left middle meatus
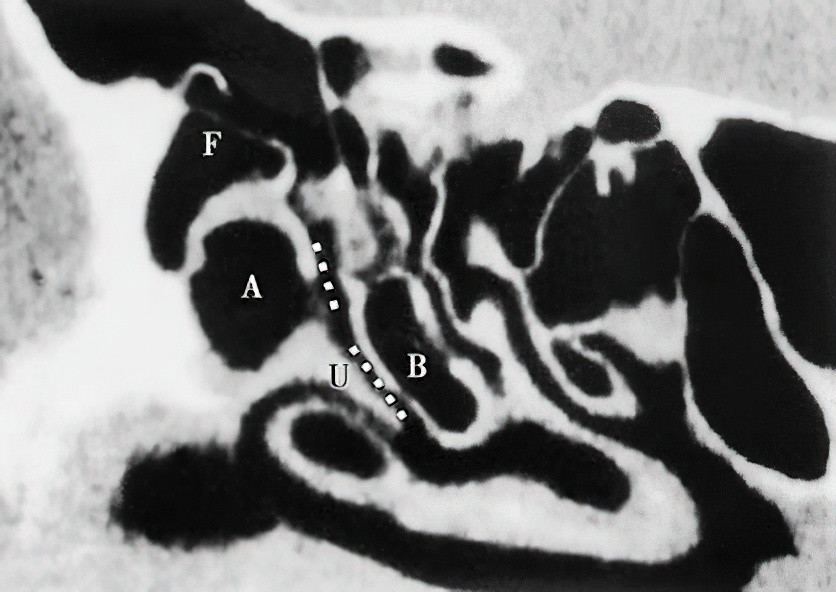
Figure 14 Sagittal CT of the nose, dashed lines indicating the ethmoidal infundibulum
F: Frontal recess
A: Agger nasi air cell
B: Bulla ethmoidalis
U: Uncinate process
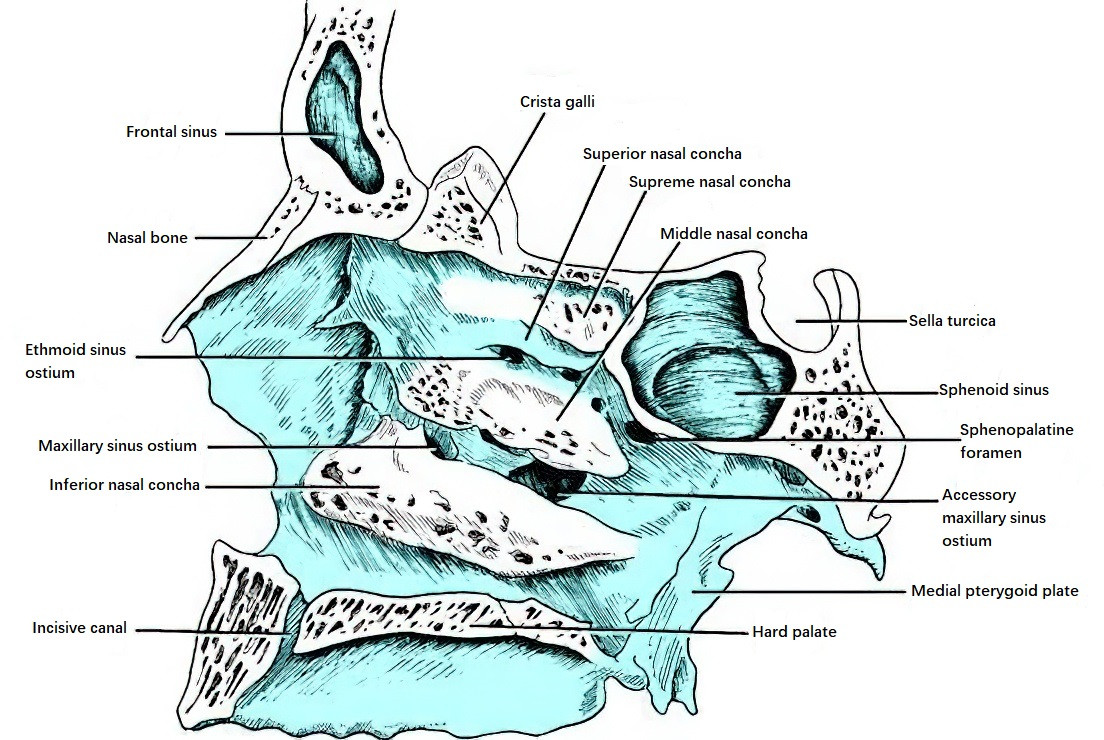
Figure 15 Lateral wall of the middle meatus
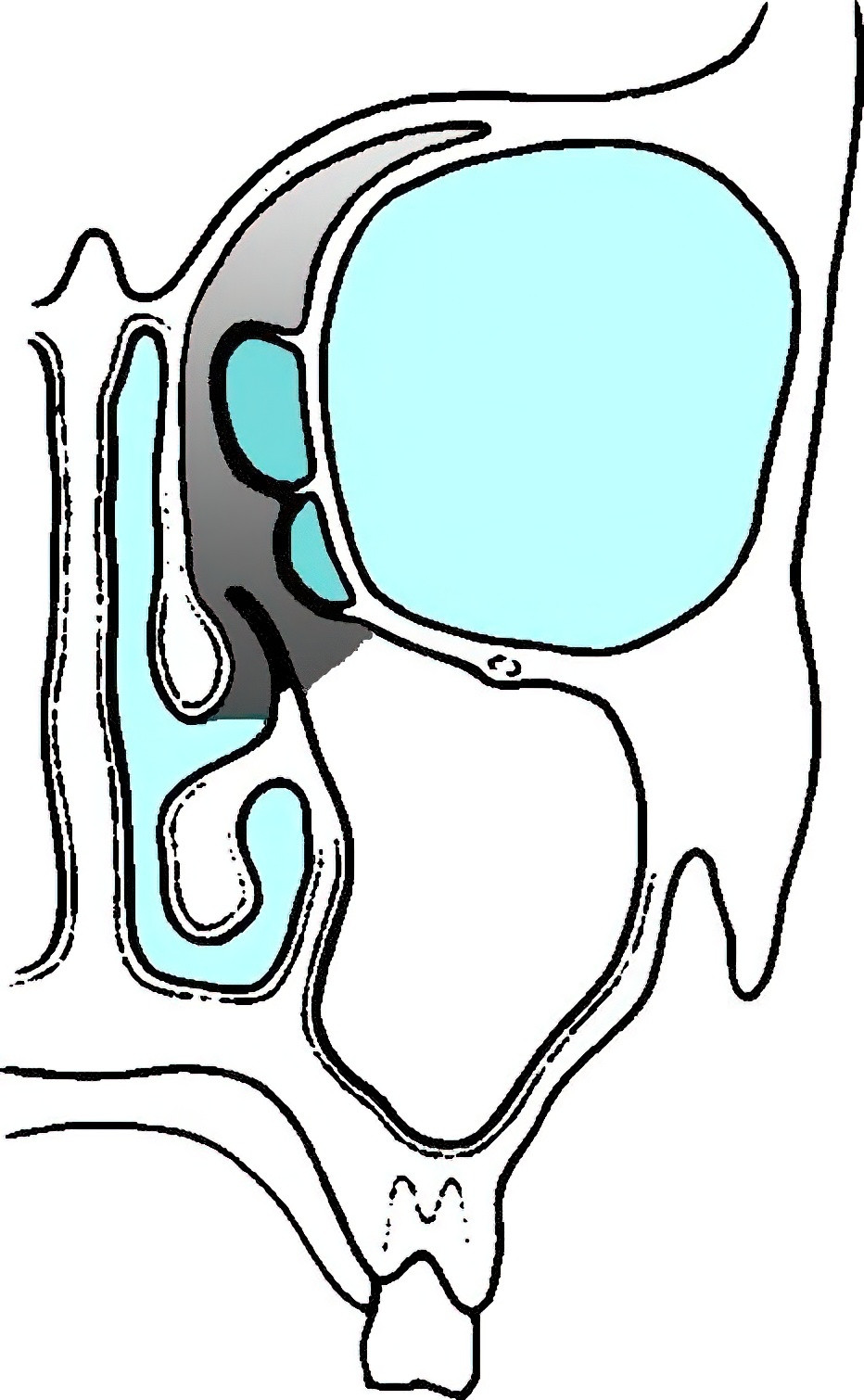
Figure 16 Schematic representation of the osteomeatal complex (Shaded area)
The semilunar hiatus widens anteriorly, inferiorly, and laterally into a funnel-shaped space called the ethmoid infundibulum. This infundibulum, located between the lateral nasal wall and the uncinate process, is a three-dimensional funnel-shaped space. Medially, it communicates with the middle meatus through the semilunar hiatus. Its superior-anterior portion is called the frontal recess, where the frontal sinus opens into the anterior-superior end of the infundibulum. Further posteriorly, the anterior ethmoid cells open, followed by the opening of the maxillary sinus.
The ethmoid bulla is the largest and most consistent air cell of the anterior ethmoid sinus. It is located in the middle meatus, situated just posterior to the uncinate process and anterior to the basal lamella of the middle turbinate. The ethmoid bulla has its base on the lamina papyracea and extends medially into the middle meatus. Its superior portion can extend to the anterior cranial base, forming the posterior boundary of the frontal recess, while posteriorly it merges with the basal lamella of the middle turbinate.
The ostiomeatal complex (OMC) refers to the common drainage pathway for the anterior ethmoid sinus, maxillary sinus, and frontal sinus. The term "OMC" is a functional entity rather than an anatomical one, denoting a critical area of interconnected anatomical structures centered around the ethmoid infundibulum. The OMC includes the middle turbinate, uncinate process, ethmoid bulla, semilunar hiatus, and the natural openings of the frontal sinus, anterior ethmoid cells, and maxillary sinus. Abnormalities or localized inflammation in this region can disrupt functionality and lead to conditions such as rhinosinusitis.
Superior turbinate and Superior Meatus, Supreme Turbinate and Supreme Meatus
The superior turbinate and the superior meatus, as well as the supreme turbinate and the supreme meatus (when present), are additional structures. The superior turbinate is the smallest of the three turbinates and is part of the ethmoid bone. It is located in the posterior-superior portion of the lateral nasal wall and sometimes appears as no more than a mucosal fold. The posterior ethmoid cells open into the superior meatus. Occasionally, a fourth turbinate known as the supreme turbinate appears superiorly-posteriorly to the superior turbinate. The space between the supreme turbinate and the superior turbinate is referred to as the supreme meatus, which may contain openings for the posterior ethmoid cells. The depression between the supreme turbinate or superior turbinate and the body of the sphenoid bone is called the sphenoethmoidal recess, where the opening of the sphenoid sinus is located.
Nasal Mucosa
The nasal mucosa consists of the olfactory region and the respiratory region, with the former accounting for approximately one-third of the nasal mucosa in adults.
Olfactory Region Mucosa
The olfactory mucosa is distributed on the medial surface of the superior turbinate, the inferior surface of the cribriform plate, the superior portion of the vertical part of the middle turbinate's medial surface, and the corresponding upper part of the nasal septum. Each side has an area of about 1 cm². The olfactory epithelium consists of two layers: the mucosal layer and the lamina propria. The mucosal layer is a pseudostratified columnar epithelium without cilia and is composed of four types of cells: olfactory sensory neurons, supporting cells, basal cells, and microvillus cells. The lamina propria contains Bowman's glands, olfactory nerve bundles, olfactory ensheathing cells, and blood vessels.
The olfactory sensory neurons are bipolar neurons with olfactory cilia. On the apical side, their dendrites extend rod-like structures toward the surface, terminating in bulbous structures called olfactory knobs. These knobs are covered with immotile cilia, where odorant receptors are located. The axons of these neurons pass into the lamina propria, where they are surrounded by olfactory ensheathing cells, forming olfactory nerve fibers. These fibers traverse the cribriform foramina to enter the olfactory bulb, with approximately 15–20 fibers per side of the nasal cavity. Bowman's glands are the primary source of mucus in the olfactory region, secreting their contents onto the epithelial surface through ducts. This mucus contains defensive compounds and odorant-binding proteins that aid in odor detection. The mucus also provides a microenvironment for the olfactory receptors, dendritic terminals, and cilia, serving as a solvent to facilitate the diffusion of odorant molecules to the receptor sites.
Respiratory Region Mucosa
The respiratory region mucosa is primarily composed of four types of cells: ciliated columnar epithelial cells, non-ciliated columnar epithelial cells, goblet cells, and basal cells. Ciliated columnar epithelial cells make up 20% to 50% of the epithelial cells, with each cell bearing approximately 250–300 cilia on its surface. The cilia measure 5–10 μm in length and about 250 nm in thickness. They are characterized by the typical "9+2" microtubule arrangement (nine pairs of peripheral microtubules and two central microtubules) along with dynein arms. Under normal physiological conditions, the cilia beat posteriorly toward the nasopharynx, performing approximately 1,000 strokes per minute and playing a central role in mucociliary clearance. Columnar epithelial cells also bear microvilli on their apical surface. Goblet cells, along with submucosal serous and mucous glands, produce mucus.
The nasal secretions form a mucociliary blanket on the mucosal surface that moves posteriorly with ciliary motion. This blanket consists of an outer mucin layer and an inner aqueous layer that supports ciliary movement. It provides a protective barrier for the nasal mucosa.
The characteristic features of nasal mucosal blood vessels include discontinuous endothelial basement membranes (facilitating material exchange), the absence of an elastic layer in the walls of small arteries (making them sensitive to chemical stimuli), and the formation of sponge-like cavernous sinusoids between arterioles and venules, which enable reflexive engorgement.
Blood Supply of the Nasal Cavity
Arterial Supply of the Nasal Cavity
The arterial supply primarily comes from branches of the ophthalmic artery (a branch of the internal carotid artery) and branches of the maxillary artery (a branch of the external carotid artery). Additional contributions are made by branches of the facial artery.
Ophthalmic Artery
After entering the orbit through the optic canal, the ophthalmic artery gives rise to the anterior ethmoid artery and posterior ethmoid artery. These arteries pass through their respective anterior and posterior ethmoidal foramina to reach the ethmoid sinuses, where they traverse grooves or canals formed by bony ridges. Eventually, they leave the sinuses to enter the anterior cranial fossa and then descend through the cribriform plate into the nasal cavity.
- The anterior ethmoid artery supplies the anterior ethmoid sinuses, frontal sinus, as well as the upper anterior portions of the lateral nasal wall and nasal septum.
- The posterior ethmoid artery supplies the posterior ethmoid sinuses and the posterior superior portions of the lateral nasal wall and nasal septum.
Maxillary Artery
Within the pterygopalatine fossa, the maxillary artery gives rise to the sphenopalatine artery, infraorbital artery, and greater palatine artery, which supply the nasal cavity. The sphenopalatine artery is the main blood supply to the nasal cavity. After passing through the sphenopalatine foramen into the nasal cavity, it divides into lateral and medial branches:
- Lateral Branch: Forms the lateral posterior nasal branches, which further divide into branches for the inferior, middle, and superior turbinates, supplying the posterior, inferior portions of the lateral nasal wall and nasal floor.
- Medial Branch: Forms the nasopalatine artery, which runs anteroinferiorly to the posterior part of the nasal septum, where it gives rise to the posterior septal nasal arteries that supply the posterior and inferior portions of the nasal septum.
Connections between the nasopalatine artery, anterior ethmoid artery, posterior ethmoid artery, superior labial artery, and greater palatine artery form an arterial plexus in the anteroinferior part of the nasal septum. This plexus is known as the Little's arterial plexus, located in an area referred to as Little's area, which is the most common site for epistaxis (nosebleeds).
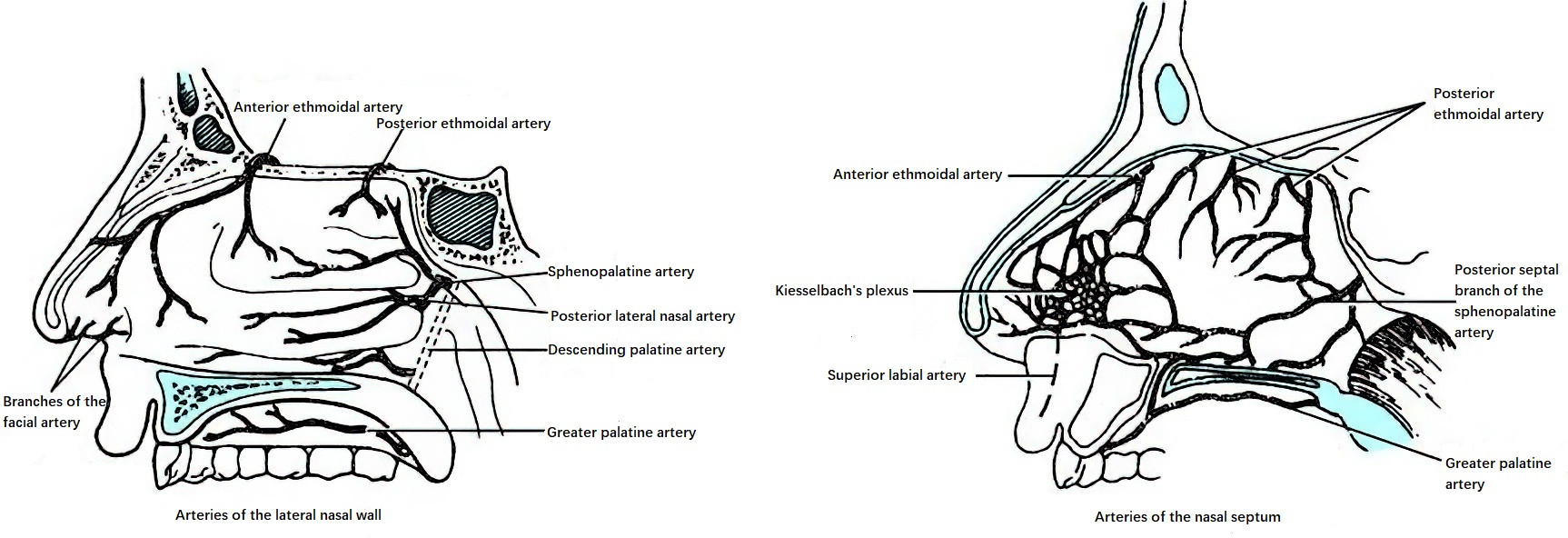
Figure 17 Arterial supply of the nasal cavity
The infraorbital artery passes through the infraorbital canal along the orbital floor before emerging at the infraorbital foramen to supply the anterior part of the lateral nasal wall. The greater palatine artery exits through the greater palatine foramen and travels anteromedially along the hard palate to enter the incisive canal, where it supplies the anteroinferior nasal septum. The superior labial artery, which originates from the facial artery, contributes to the formation of Little's arterial plexus.
Venous Drainage of the Nasal Cavity
The veins of the anterior, posterior, and inferior nasal regions drain into the internal and external jugular veins. The veins of the superior nasal region drain via the ophthalmic veins into the cavernous sinus and may also drain intracranially through the ethmoidal veins into dural sinuses such as the superior sagittal sinus. The anteroinferior nasal septum contains a venous plexus known as the Kiesselbach plexus, which is an important source of bleeding in this area.
In elderly individuals, a superficial and dilated venous plexus located near the nasopharynx and the lateral wall of the inferior meatus is referred to as Woodruff's naso-nasopharyngeal venous plexus. This plexus is a common bleeding source in the posterior nasal cavity.
From an anatomical perspective, the arterial and venous vascular networks formed in the anteroinferior nasal septum by branches of the internal and external carotid systems can be referred to as the Little’s arterial plexus and the Kiesselbach venous plexus, respectively. Clinically, this area is known as the "bleeding zone."
Nasal Lymphatics
The lymphatic vessels in the anterior one-third of the nasal cavity are connected to the lymphatic vessels of the external nose and drain into the anterior auricular lymph nodes, parotid lymph nodes, and submandibular lymph nodes. The lymphatic drainage from the posterior two-thirds of the nasal cavity flows into the retropharyngeal lymph nodes and the upper deep cervical lymph nodes. Malignant tumors of the nasal cavity can spread to lymph nodes along these pathways.
Nasal Innervation
Olfaction is transmitted by the olfactory nerve, while general sensations of the nasal mucosa (such as touch, pain, and temperature) are carried by branches of the ophthalmic nerve and maxillary nerve, which are divisions of the trigeminal nerve. Autonomic nerves are distributed to the mucosal glands and regulate vascular tone and glandular secretion.
Olfactory Nerves (Cranial Nerve I)
The olfactory nerves are specialized visceral sensory nerves dedicated to transmitting olfactory information from the nasal cavity to the brain. These nerves originate from olfactory receptor cells located in the olfactory mucosa in the upper part of the nasal cavity. These bipolar neurons congregate to form approximately 20 olfactory filaments, which pass through the foramina in the cribriform plate of the ethmoid bone and the dura mater to reach the anterior cranial fossa and terminate in the olfactory bulb. In the olfactory bulb, olfactory nerve fibers synapse with mitral cells to form synaptic structures. Fibers from olfactory bulb neurons travel through the olfactory tract and terminate in the olfactory centers of the brain, including the piriform cortex of the temporal lobe, anterior hippocampal gyrus, and amygdala. Some fibers also terminate in the subcallosal gyrus or the anterior perforated substance through the medial and intermediate olfactory striae, facilitating reflex connections of olfaction. The conduction pathway includes olfactory receptor cells in the olfactory mucosa → olfactory nerve fibers (olfactory filaments, fila olfactoria) passing through the cribriform plate → olfactory bulb → olfactory tract → olfactory centers in the forebrain, which govern the sense of smell. The sheath of the olfactory nerve is a continuation of the dura mater, and damage to the olfactory mucosa or secondary infections may allow pathogens to travel along the olfactory nerve sheath, potentially leading to intracranial complications secondary to nasal disease.
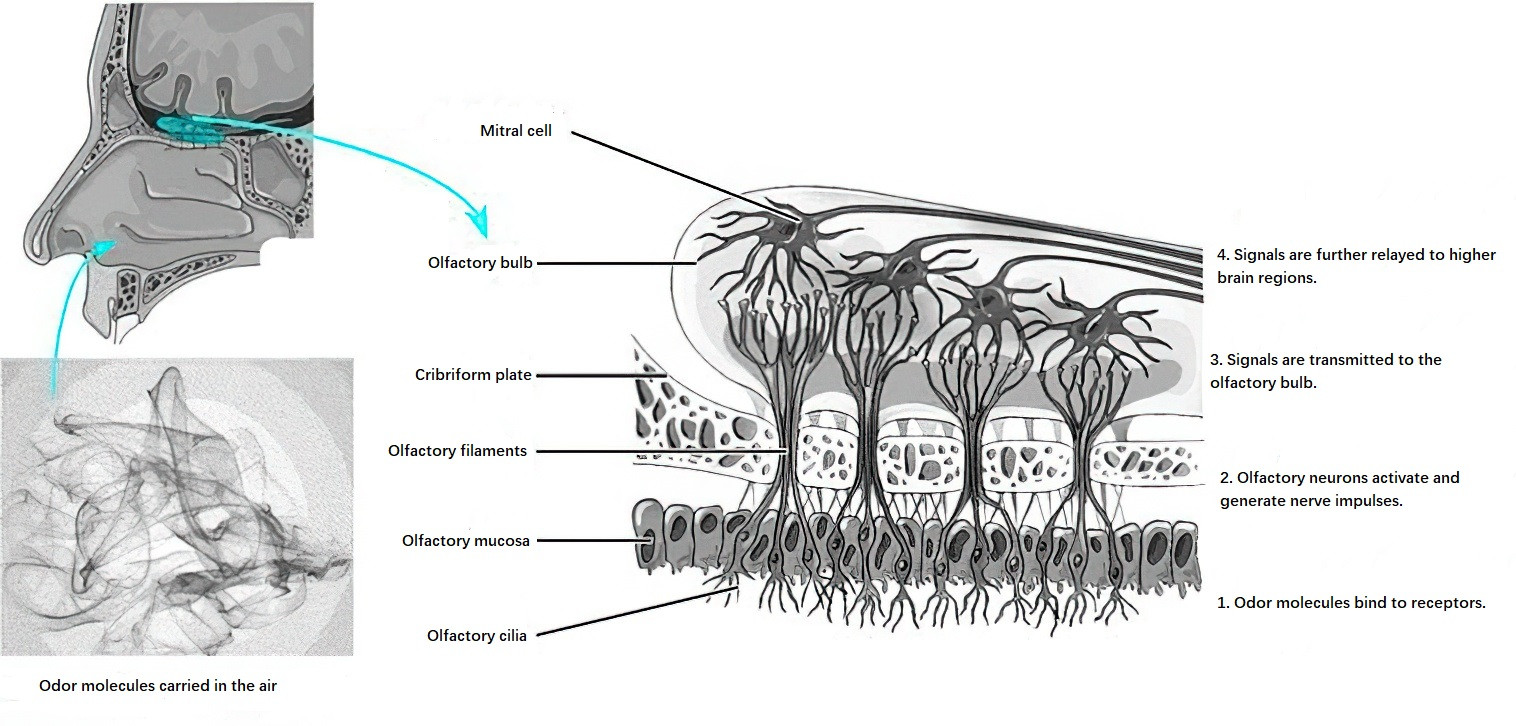
Figure 18 Olfactory signal transduction pathway
Sensory Nerves
Sensory innervation comes from branches of the ophthalmic nerve (first division of the trigeminal nerve) and the maxillary nerve (second division of the trigeminal nerve).
Ophthalmic Nerve (V1)
The ophthalmic nerve gives off the nasociliary nerve, which then branches into the anterior ethmoidal nerve and posterior ethmoidal nerve. These nerves travel alongside their corresponding arteries. Upon entering the nasal cavity, the anterior ethmoidal nerve divides into medial and lateral branches, with the medial branch innervating the upper anterior portion of the nasal septum and the lateral branch innervating the upper lateral nasal wall and external nasal skin. The posterior ethmoidal nerve provides sensory innervation to the nasal septum and the olfactory region.
Maxillary Nerve (V2)
After passing through or around the pterygopalatine ganglion (also known as Meckel's ganglion), the maxillary nerve gives rise to the pterygopalatine nerves, which enter the nasal cavity via the sphenopalatine foramen. These nerves divide into posterior superior lateral nasal branches and posterior superior medial nasal branches, innervating the posterior parts of the lateral nasal wall, the roof of the nasal cavity, and the nasal septum. The posterior superior medial nasal branch also gives rise to the nasopalatine nerve, which runs obliquely along the posterior superior nasal septum.
Additional branches of the pterygopalatine nerve, such as the palatine nerves, also give rise to the anterior palatine nerve (also called the greater palatine nerve). After passing through the pterygopalatine canal, these nerves further branch into posterior inferior nasal nerves, innervating the middle meatus, inferior turbinate, and inferior meatus. The maxillary nerve also gives rise to the infraorbital nerve, which has branches that supply the nasal vestibule, the maxillary sinus, the nasal floor, and the anterior part of the inferior meatus.
Autonomic Nerves
The vasomotor tone of the nasal mucosal blood vessels and secretions of the mucosal glands are regulated by autonomic nerves. Sympathetic fibers originate from the deep petrosal nerve, which arises from the carotid sympathetic plexus surrounding the internal carotid artery. Parasympathetic fibers originate from the greater superficial petrosal nerve, a branch of the facial nerve. Both the deep petrosal nerve and greater superficial petrosal nerve merge within the pterygoid canal to form the vidian nerve, which traverses the base of the middle cranial fossa, passes beneath the floor of the sphenoid sinus, and exits at the root of the pterygoid process to reach the pterygopalatine ganglion in the pterygopalatine fossa. Postganglionic fibers from this ganglion innervate the nasal cavity.
Sympathetic fibers do not synapse within the pterygopalatine ganglion and primarily mediate vasoconstriction in the nasal mucosa. Parasympathetic fibers do synapse within the ganglion, and the postganglionic fibers travel with branches of the maxillary nerve (such as the posterior nasal nerves) to reach the nasal mucosa, where they mediate vasodilation and glandular secretion. The nasal mucosa contains abundant sympathetic and parasympathetic fibers, and under normal conditions, these autonomic systems maintain a dynamic balance.
Paranasal Sinuses
The paranasal sinuses are paired structures located bilaterally, consisting of four pairs named after the bones in which they reside: the maxillary sinuses, ethmoid sinuses, frontal sinuses, and sphenoid sinuses. The development of these sinuses occurs later than that of the nasal cavity and is primarily completed after birth. Based on the location and drainage direction of their natural openings, the sinuses are classified into anterior and posterior groups. The anterior group includes the maxillary sinuses, anterior ethmoid sinuses, and frontal sinuses, which all drain into the middle meatus. The posterior group includes the posterior ethmoid sinuses and sphenoid sinuses, with the former draining into the superior or supreme meatus and the latter opening into the sphenoethmoidal recess located above and behind the superior turbinate. The sinus mucosa is continuous with the nasal mucosa, allowing inflammation to spread between these regions.
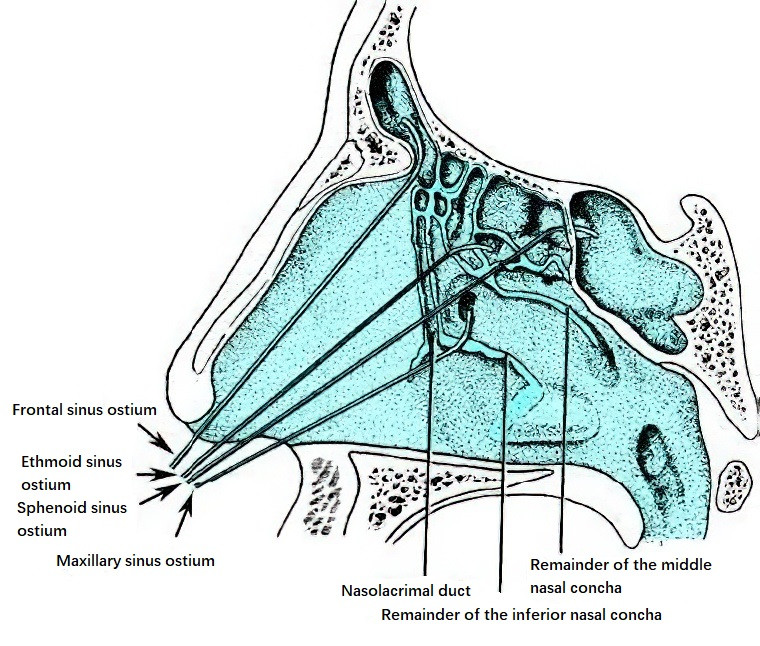
Figure 19 Sinus ostia locations
Maxillary Sinus
The maxillary sinus, located within the body of the maxilla, is the largest of the paranasal sinuses, with an average volume of approximately 13 mL. It has an irregular pyramidal shape, with its base forming the lateral wall of the nasal cavity and its apex pointing toward the zygomatic process of the maxilla. The maxillary sinus has five walls:
- Anterior Wall: Thin and slightly concave at its center, forming the canine fossa. Above the canine fossa and approximately 12 mm below the infraorbital margin, the infraorbital foramen is situated, through which the infraorbital nerve and vessels pass.
- Posterior Wall: Located adjacent to the pterygopalatine fossa and the infratemporal fossa. In cases of malignant maxillary sinus tumors, invasion of this wall can involve the medial pterygoid muscle, leading to trismus.
- Medial Wall: Forming the lower part of the lateral wall of the nasal cavity, it is relatively thick near the nasal cavity floor and becomes thinner superiorly. The attachment site of the inferior turbinate is particularly thin, making it an ideal location for puncture of the maxillary sinus through the inferior meatus. The natural opening of the maxillary sinus is located in the upper anterior part of the medial wall. The bony opening, known as the maxillary hiatus, is divided into four quadrants by the uncinate process and the ethmoidal process of the inferior turbinate. Only the anterosuperior quadrant serves as the true natural ostium, while the other quadrants are sealed by a double layer of mucosa and dense connective tissue, referred to as the nasal fontanelle. The diameter of the natural ostium averages 2.8 mm.
- Superior Wall: Forms the floor of the orbit. This thin wall is traversed by the infraorbital canal, which transmits the infraorbital nerve and vessels to the infraorbital foramen and the canine fossa. Fractures of the orbital floor can result in restricted ocular movements, diplopia, or enophthalmos.
- Inferior Wall: Corresponds to the alveolar process of the maxilla and lies below the floor of the nasal cavity. This wall is closely related to the roots of the second premolar and the first and second molars, which are often separated from the sinus cavity by only a thin layer of bone. Infection of these teeth can easily spread into the sinus, leading to odontogenic maxillary sinusitis.
Ethmoid Sinus
The ethmoid sinuses, located within the ethmoid bone in the superolateral portion of the nasal cavity, are situated between the orbits and anterior to the sphenoid sinus, below the anterior cranial fossa. They consist of honeycomb-like air cells and are the most anatomically complex, variable, and closely related to adjacent structures among all paranasal sinuses. For this reason, the ethmoid sinuses are also referred to as the "ethmoid labyrinth." They are divided into anterior ethmoid sinuses and posterior ethmoid sinuses by the basal lamella of the middle turbinate.
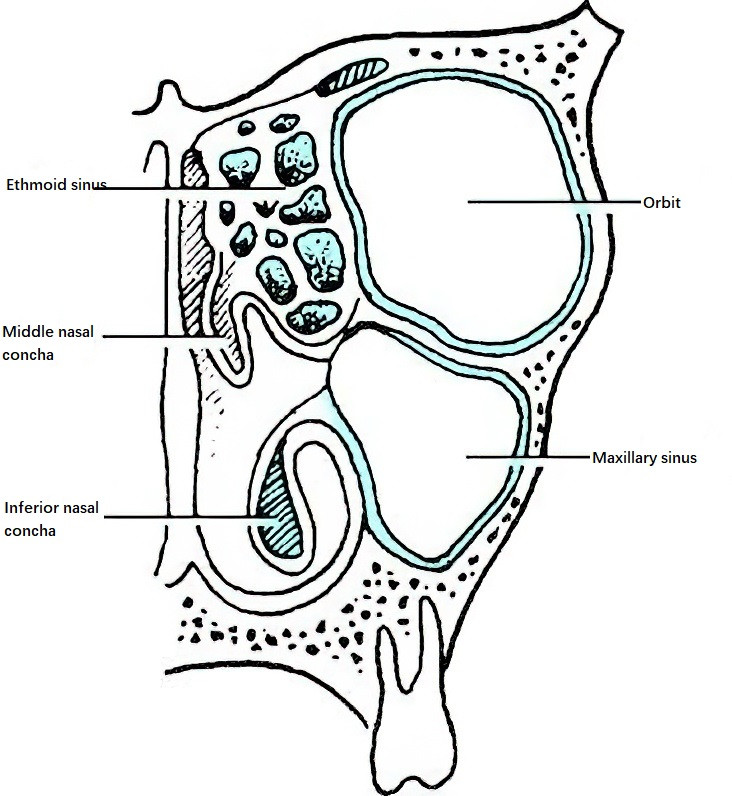
Figure 20 Relationship between maxillary sinus, ethmoid sinus, and orbit
The ethmoid sinuses have six walls:
- Lateral Wall: Forming the medial wall of the orbit, this wall is primarily composed of the lacrimal bone and the lamina papyracea. Damage to the lamina papyracea during surgery can result in orbital complications. Notably, the lamina papyracea aligns with the medial wall of the maxillary sinus on the same sagittal plane.
- Medial Wall: Representing the upper part of the lateral nasal wall, this wall houses the superior and middle turbinates.
- Superior Wall: Medially connected to the horizontal plate of the ethmoid bone and laterally continuous with the roof of the orbit. The anterior cranial fossa lies immediately above the ethmoid roof. The connection between the ethmoid roof and the cribriform plate can take two forms: (1) A "platform" or "inclined" type, in which the ethmoid roof and cribriform plate meet at nearly the same level or with a gradual slope; (2) A "stepped" type, where the cribriform plate lies significantly lower than the ethmoid roof, creating a steep recess called the ethmoid fovea. The medial wall of this recess is extremely thin and can be vulnerable to damage during surgery, potentially resulting in anterior cranial fossa injury or cerebrospinal fluid leakage. The anterior ethmoidal artery is a key landmark in the ethmoid roof.
- Inferior Wall: Formed by structures of the middle meatus lateral wall, including the ethmoidal bulla, uncinate process, and ethmoid infundibulum.
- Anterior Wall: Made up of the ethmoidal notch of the frontal bone, the nasal crest, and the frontal process of the maxilla. A notable structure in this area is the frontal recess.
- Posterior Wall: Formed by the sphenoethmoidal junction, adjacent to the sphenoid sinus. In cases of extensive pneumatization, the most posterior ethmoid air cells can extend above the sphenoid sinus, forming suprasphenoid cells. If the optic nerve canal protrudes into the lateral wall of the most posterior ethmoid air cell, it creates a prominence known as the optic nerve tubercle. Ethmoid air cells associated with this prominence are termed Onodi cells. In well-pneumatized cases, the posterior ethmoid air cells can also abut the internal carotid artery, creating depressions within the sinus wall.
Frontal Sinus
The frontal sinuses, located between the inner and outer tables of the frontal bone, are paired structures. The sinuses progressively narrow as they course downward and inward, with the narrowest region occurring at the ostium located at the base of the sinus. The frontal process of the maxilla at the anterior wall of the frontal sinus determines the size of the ostium, forming an anatomical landmark referred to as the "nasal crest" or "frontal beak."
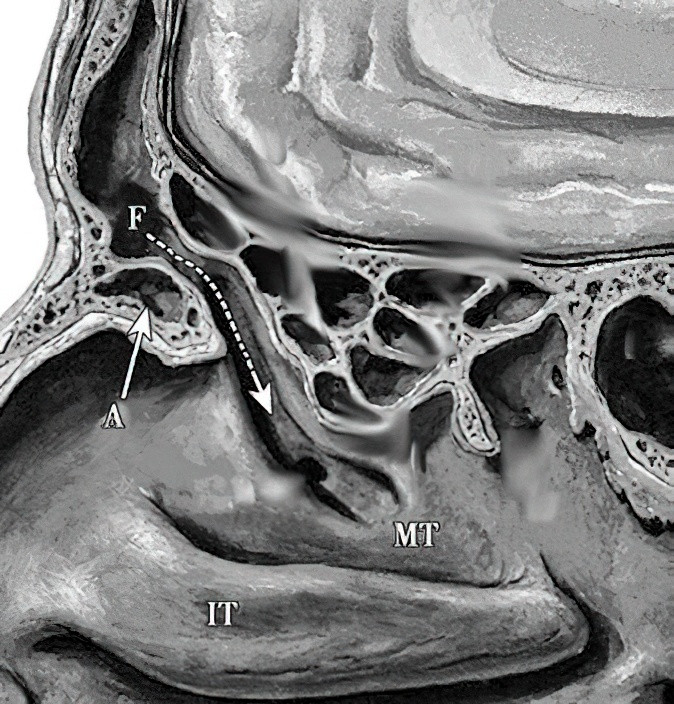
Figure 21 Anatomy of the frontal recess
F: Frontal sinus
A: Agger nasi
IT: Inferior nasal concha
MT: Middle nasal concha
Dashed lines indicate the drainage pathway of the frontal sinus.
The frontal sinus has four walls:
- Anterior Wall: Composed of the outer plate of the frontal bone, this wall is thick and contains marrow. Frontal sinusitis can lead to osteomyelitis of this wall.
- Posterior Wall: The inner plate of the frontal bone, which is thinner and forms part of the anterior wall of the anterior cranial fossa. Venous drainage from the sinus mucosa penetrates this wall to connect with dural venous sinuses, making intracranial invasion possible in cases of infection.
- Inferior Wall: Primarily forming the roof of the orbit (external three-quarters) and the roof of the anterior ethmoid sinuses (inner quarter). The bone in this region is thin, especially in the superomedial corner of the orbit. Acute frontal sinusitis can cause tenderness in this area and may lead to subperiosteal abscesses in the superomedial orbital wall.
- Medial Wall: The bony partition separating the left and right frontal sinuses, often deviating toward one side.
The frontal sinus ostium transitions inferiorly into the frontal recess. The frontal beak, located at the posterior portion of the anterior frontal sinus wall, forms the anterior border of the sinus ostium, while the skull base forms its posterior border. The lateral boundary is the orbital lamina, while the medial boundary comprises the vertical plate of the middle turbinate and the lateral nasal wall of the olfactory cleft. The frontal recess resembles the lower half of an hourglass in the sagittal plane, with the upper portion opening into the frontal sinus. Adjacent ethmoid air cells, such as the agger nasi cells and frontal ethmoid cells, can alter drainage patterns in this region. Among these cells, the agger nasi is a consistent anatomical structure.
Sphenoid Sinus
The sphenoid sinus is located posterior, medial, and inferior to the posterior ethmoid sinuses, occupying the body of the sphenoid bone. Due to variations in the degree of pneumatization and the position of the sphenoid sinus septum, the size, shape, and volume of the left and right sinus cavities can differ. The average size of the sphenoid sinus is approximately 2 cm × 2 cm × 3 cm, with a volume ranging from 5.8 to 7.5 mL. The walls of the sphenoid sinus, particularly the lateral, superior, and posterior walls, have complex anatomical relationships with adjacent structures.
- Lateral Wall: This wall is adjacent to the middle cranial fossa, the cavernous sinus, the internal carotid artery, and the optic nerve canal. In well-pneumatized sphenoid sinuses, the lateral wall may be extremely thin or even dehiscent, leaving these structures exposed within the sinus cavity. Surgical procedures in this area need to account for the potential risk of damage to the optic nerve or the internal carotid artery, which could result in blindness or fatal hemorrhage.
- Superior Wall: Above this wall lies the floor of the middle cranial fossa, which has a saddle-like configuration known as the sella turcica. The sella turcica houses the pituitary gland.
- Anterior Wall: This wall contributes to the posterior section of the nasal roof and the posterior wall of the ethmoid sinus (sphenoethmoidal plate). The natural opening of the sphenoid sinus is located in the anterosuperior portion of the anterior wall, near the nasal septum or the sphenoidal crest, and opens into the sphenoethmoidal recess.
- Posterior Wall: This thicker wall forms part of the clivus.
- Inferior Wall: This wall corresponds to the superior margins of the choanae and the roof of the nasopharynx.
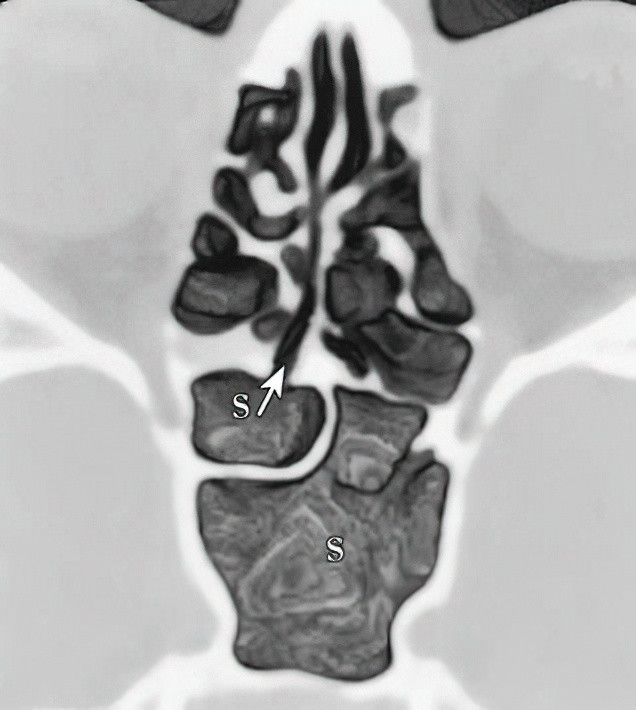
Figure 22 Axial CT of the nose, highlighting the opening of the sphenoid sinus (S) (Arrow)
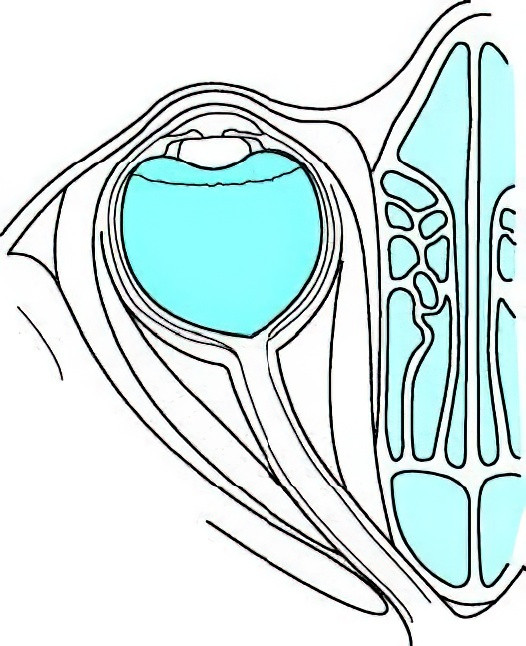
Figure 23 Anatomy of the optic canal
The relationships between the sphenoid sinus and the optic nerve canal, the internal carotid artery, and the cavernous sinus are significant:
- Relationship with the Optic Nerve Canal: The lateral wall of the sphenoid sinus and its proximity to the optic nerve canal depend on the extent of pneumatization and development of the posterior ethmoid and sphenoid sinuses. When the posterior ethmoid air cells are well-developed and extend into the sphenoid sinus, and an optic nerve canal prominence is present, attention to identification and protection of these structures is critical during surgical interventions.
- Relationship with the Internal Carotid Artery (ICA) Prominence: The cervical segment of the ICA begins at the bifurcation of the common carotid artery, ascends to the base of the skull, and enters the cranium through the carotid canal in the petrous part of the temporal bone. The ventral skull base trajectory of the ICA is divided into six segments (proximodistally): the parapharyngeal segment, petrous segment, clival segment, parasellar segment, clinoidal segment, and intradural segment. The carotid sulcus, a shallow groove on the lateral wall of the sphenoid body, accommodates the cavernous segment of the ICA. Within well-pneumatized sphenoid sinuses, the carotid sulcus forms a bony elevation on the lateral wall beneath the sellar floor, referred to as the ICA prominence. This prominence is subdivided into the posterior sellar segment (transition between the petrous and proximal cavernous segments), the sellar segment (horizontal portion of the cavernous segment), and the anterior sellar segment (located near the anterior wall of the sphenoid sinus). Among these, the posterior and anterior sellar segments are thinner, with the thinnest portion found at the anterior sellar segment below the tuberculum sellae. In well-developed sphenoid sinuses, the bone over the ICA prominence may be extremely thin or even dehiscent.
- Relationship with the Cavernous Sinus: The cavernous sinus is a venous sinus formed by the dura mater, situated bilaterally to the sphenoid sinus and the sella turcica. It contains the internal carotid artery and cranial nerves III (oculomotor nerve), IV (trochlear nerve), V (trigeminal nerve, specifically its ophthalmic and maxillary divisions), and VI (abducens nerve). When the lateral wall of the sphenoid sinus is damaged or congenitally dehiscent, the cavernous sinus may protrude into the sphenoid sinus cavity.
Blood Supply, Lymphatic Drainage, and Innervation of the Paranasal Sinuses
Blood Supply
The blood supply to the maxillary sinus is primarily provided by the posterior superior alveolar artery, the infraorbital artery, and the posterior lateral nasal artery, with venous drainage occurring through the sphenopalatine vein. The ethmoid sinuses receive arterial blood from the anterior ethmoidal artery, the posterior ethmoidal artery, the supraorbital artery, and the posterior lateral nasal artery. Venous drainage occurs through the anterior and posterior ethmoidal veins, with potential drainage into veins of the dura mater, as well as the venous plexuses of the olfactory bulb and frontal lobe.
The arterial supply to the frontal sinus is derived from the anterior ethmoidal artery, the supraorbital artery, and the posterior lateral nasal artery. Venous drainage occurs through the ethmoidal veins, with additional drainage via the diploic veins and veins of the dura mater into the sagittal sinus.
The sphenoid sinus is supplied by small branches of the ascending pharyngeal artery (a branch of the external carotid artery), the pharyngeal branches of the maxillary artery, and branches of the sphenopalatine artery. Venous drainage occurs through the sphenopalatine vein, with some venous connections to the cavernous sinus.
Lymphatic Drainage
The paranasal sinuses have relatively few capillary lymphatic vessels, which primarily drain into the retropharyngeal lymph nodes and the upper group of the deep cervical lymph nodes.
Sensory Innervation
The sensory innervation of all paranasal sinuses is predominantly provided by the first (ophthalmic) and second (maxillary) divisions of the trigeminal nerve.