Acoustic immittance testing, also known as acoustic impedance testing, is one of the most commonly used objective hearing tests in clinical practice. Changes in external auditory canal pressure alter the tension of the tympanic membrane, thereby changing its ability to transmit sound energy. This property allows for the measurement of sound energy reflected back into the external auditory canal, which provides an assessment of the function of the middle ear sound transmission system and the auditory brainstem pathway. Acoustic immittance encompasses both acoustic admittance and acoustic impedance. Acoustic impedance refers to the resistance encountered by sound waves as they move medium molecules, expressed as the ratio of sound pressure exerted on a unit area to the effective volumetric velocity through that plane. Acoustic admittance, on the other hand, is the sound energy absorbed and transmitted by the medium and is the reciprocal of acoustic impedance. Under constant sound intensity, a greater acoustic impedance of a medium results in lower acoustic admittance. The acoustic immittance of a medium depends on its friction (resistance), mass (inertia), and stiffness (elasticity). The mass of the middle ear transmission system, which includes the weight of the tympanic membrane and ossicles, remains relatively constant. The ossicular chain, suspended by muscles and ligaments, experiences minimal frictional resistance. Stiffness, which is determined by the elasticity of the tympanic membrane, ossicular chain, and middle ear air cushion, is more variable and is the primary determinant of middle ear admittance. As such, acoustic immittance devices primarily measure the stiffness of the tympanic membrane and ossicular chain to assess the acoustic immittance of the entire middle ear system.
Middle Ear Immittance Devices, often referred to in clinical settings as acoustic impedance meters, operate based on the principle of equivalent ear canal volume. These devices include two main components: an admittance bridge and a stimulus signal generator. The admittance bridge introduces three small tubes, sealed within the external auditory canal using a probe. The upper tube emits a probe tone of 220 Hz or 226 Hz at 85 dB to observe dynamic changes in tympanic admittance as pressure varies. It also generates pure tone signals, white noise, and narrowband noise stimuli, with intensities of 40–125 dB and test frequencies of 250 Hz, 500 Hz, 1,000 Hz, 2,000 Hz, and 4,000 Hz, to assess ipsilateral or contralateral acoustic reflexes of the stapedius muscle. The lower tube captures sound energy reflected by the tympanic membrane into the external auditory canal, converts it into electrical signals via a microphone, and amplifies and displays it using a bridge balance meter. The middle tube is connected to an air pump that continuously varies the external auditory canal pressure from +2 kPa to -4 or -6 kPa.
Tympanometry
Tympanogram (also called acoustic admittance graph or compliance graph)
As the external auditory canal pressure transitions continuously from positive to negative, the tympanic membrane is first deflected inward, then gradually returns to its natural position, and finally bulges outward. The resulting dynamic changes in compliance are recorded in the form of a pressure-compliance function curve, referred to as the tympanogram. The curve's shape, the position of the compliance peak along the pressure axis (point of peak pressure), the height of the peak (curve amplitude), and the slope and smoothness of the curve reflect the condition of the middle ear.
- Type A Curve: Indicates normal middle ear function.
- Type As Curve: Indicates restricted mobility of the middle ear transmission system, as seen in conditions such as otosclerosis, ossicular fixation, or significant thickening of the tympanic membrane.
- Type Ad Curve: Indicates hypermobility of the tympanic membrane, as seen in ossicular discontinuity, atrophic tympanic membranes, healed perforations, or abnormal patency of the Eustachian tube.
- Type B Curve: Indicates middle ear effusion or extensive middle ear adhesions.
- Type C Curve: Indicates Eustachian tube dysfunction or negative middle ear pressure.
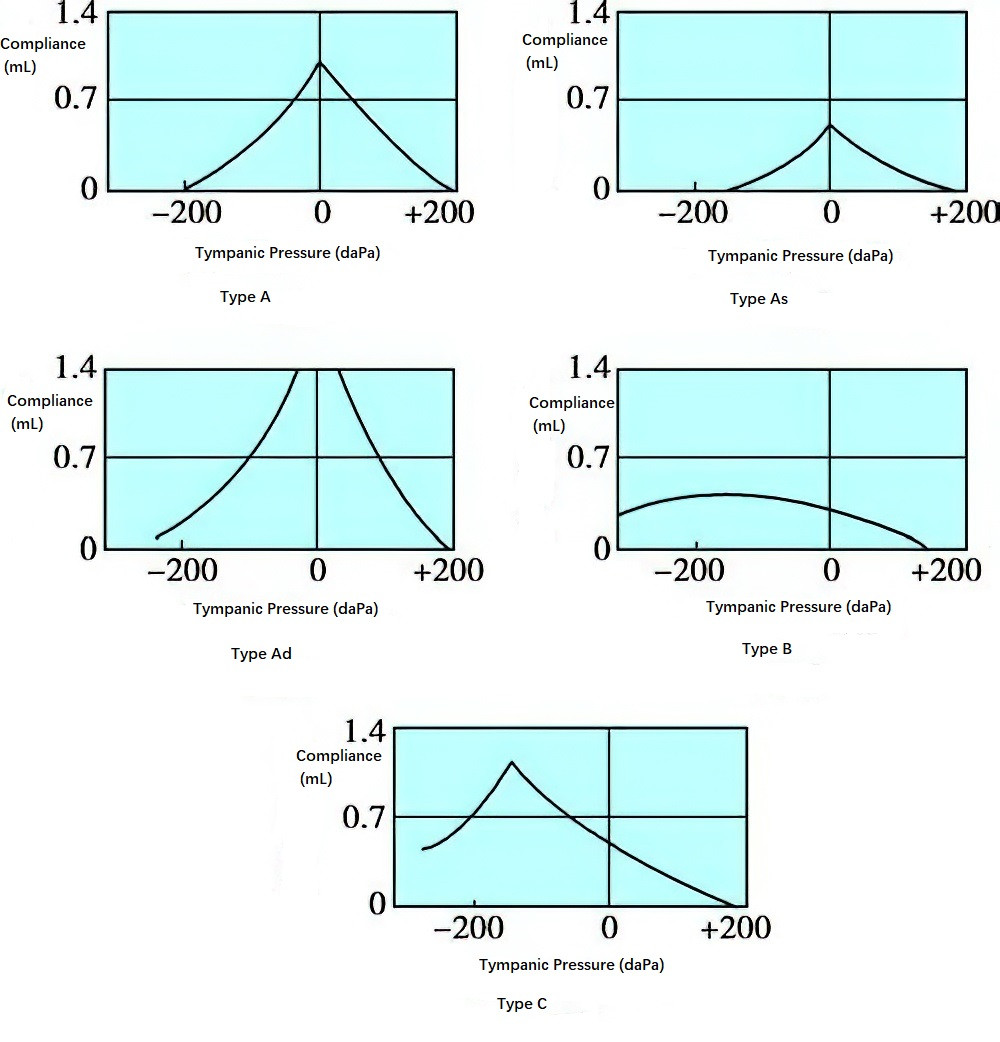
Figure 1 Tympanogram (Tympanic function curve)
Static Compliance
Static compliance refers to the difference in tympanic membrane compliance (measured in equivalent ear canal volume in milliliters) between its natural state and when it is compressed under positive pressure. This value represents the mobility of the middle ear transmission system. Because there is significant variability in normal individuals, static compliance should be interpreted alongside the results of stapedius muscle reflex tests and pure-tone audiometry.
Comparison of tympanograms before and after applying the Valsalva maneuver (nose-pinching and forced exhalation) or Toynbee maneuver (nose-pinching and swallowing) may reveal shifts in the peak pressure point. A significant shift suggests normal Eustachian tube function, whereas no shift indicates impaired function.
Stapedius Muscle Acoustic Reflex
The stapedius muscle acoustic reflex occurs when an acoustic stimulus, converted into auditory nerve impulses in the inner ear, travels via the cochlear nerve to the ventral cochlear nucleus in the brainstem. The impulse continues ipsilaterally or crosses to the contralateral superior olivary nucleus, eventually reaching the facial nerve nuclei on both sides and activating the stapedius muscles innervated by the facial nerves. Contraction of the stapedius muscles changes tympanic membrane compliance, which is recorded by the acoustic immittance device. In individuals with normal hearing, both crossed (contralateral) and uncrossed (ipsilateral) reflexes can be elicited in each ear.
The stapedius acoustic reflex has various clinical applications, including:
- Evaluating hearing sensitivity.
- Using acoustic reflex threshold and loudness recruitment to differentiate between conductive and sensorineural hearing loss.
- Applying acoustic reflex decay testing to assess auditory adaptation and differentiate between cochlear and retrocochlear hearing loss (refer to supra-threshold auditory function testing and auditory adaptation tests).
- Identifying non-organic hearing loss.
- Providing localization diagnosis and prognosis predictions for peripheral facial paralysis.
- Assisting in the diagnosis and therapeutic assessment of conditions such as myasthenia gravis.
In cases of cochlear implantation, acoustic reflex testing on the implanted side, using signals from the external device, can verify whether the stimulus signal has successfully reached the auditory nerve.