Sensorineural hearing loss is a condition caused by cochlear pathologies, while neural hearing loss is due to post-cochlear auditory nerve lesions. Together, these are classified as sensorineural hearing loss. Suprathreshold auditory function testing assists in differentiating between cochlear and retrocochlear pathologies. This testing includes the recruitment test, Short Increment Sensitivity Index (SISI) test, auditory fatigue, and pathological adaptation tests.
Recruitment Test
Sound intensity, as a physical quantity, can be measured objectively. Loudness, however, is the subjective perception of sound intensity by the human ear and depends not only on the physical intensity but also on the frequency of sound. Under normal conditions, loudness increases or decreases proportionally with sound intensity; as sound intensity increases, loudness grows, and as sound intensity decreases, loudness diminishes.
In cases of cochlear pathology, even a slight increase in sound intensity can cause abnormally rapid growth in loudness, which is referred to as the recruitment phenomenon or the phenomenon of loudness recruitment. Clinically, this manifests as auditory hypersensitivity, where the individual cannot tolerate excessively loud sounds. This phenomenon limits the dynamic range of frequency responses during cochlear implant tuning or hearing aid fitting, reducing tolerance for volume.
Alternate Binaural Loudness Balance Test (ABLB)
This test is applicable for individuals with unilateral deafness, bilateral hearing loss of differing degrees, or interaural hearing threshold differences greater than 20 dB in the mid-frequencies.
Method: A 1-kHz pure tone is selected for testing via air conduction. Hearing thresholds for both ears are recorded at this frequency. For individuals with a threshold difference greater than 20 dB between ears, sound intensity is increased alternately on both sides in fixed increments (10–20 dB per step) until the intensity of the poorer ear matches the loudness perceived by the healthier ear. The sound intensities for both ears are recorded at the point of perceived equal loudness, and a line is drawn connecting the intensity levels of the two ears.
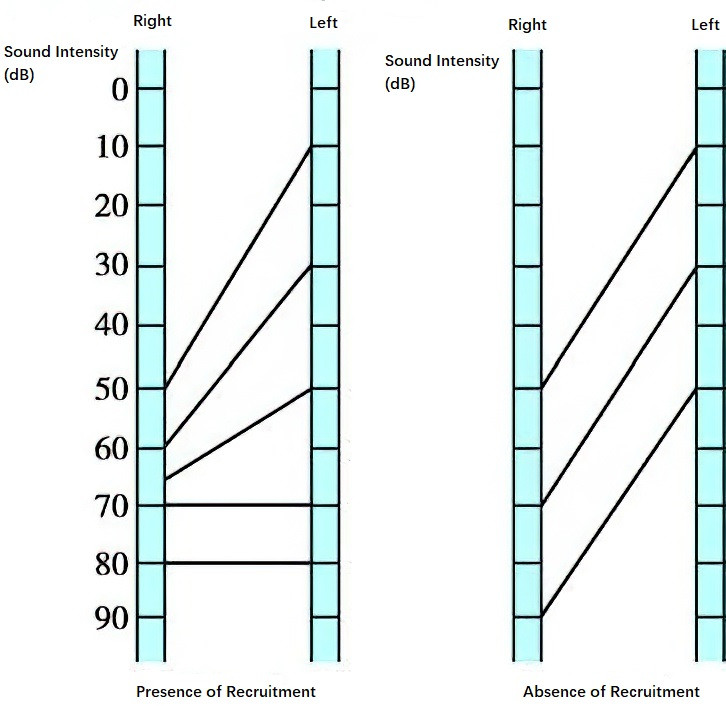
Figure 1 Loudness balance test
Gradually, the sound intensity of the better ear is increased until both ears perceive equal loudness at the same sound intensity level, despite the initial interaural threshold difference of over 20 dB. Achieving equal loudness indicates the presence of recruitment. If equal loudness is never achieved at the same sound level for both ears, recruitment is absent.
When the affected ear demonstrates slower loudness growth than the normal ear and requires greater sound intensity for loudness balance, this phenomenon is called decruitment. Decruitment is indicative of retrocochlear pathologies, such as acoustic neuroma.
Metz Recruitment Test
The difference between pure-tone hearing thresholds and stapedius muscle reflex thresholds at the same frequency is normally 75–95 dB. A difference of ≤60 dB indicates cochlear hearing loss with recruitment, while a difference of ≥100 dB suggests retrocochlear hearing loss.
Tests for Auditory Fatigue and Pathological Adaptation
Sustained exposure to high-intensity sound stimuli may result in reduced auditory sensitivity, a phenomenon known as auditory fatigue. A temporary and minor reduction in hearing, in which loudness diminishes during prolonged sound stimulation, is referred to as auditory adaptation. Collectively, these phenomena are termed tone decay.
In neural hearing loss, the severity and speed of auditory fatigue and adaptation exceed normal levels, which is referred to as pathological adaptation. Common tone decay tests include:
Pure Tone Audiometry Testing Method
One or two mid-frequency pure tones are chosen as test stimuli. During testing, continuous stimulation is provided at the hearing threshold level for the test ear. The sound remains audible for one minute. If the sound becomes inaudible within one minute, the intensity is raised by 5 dB increments until the sound is continuously audible for one minute at the same intensity level.
For normal ears and conductive hearing loss, the difference between the stimulus level and hearing threshold is 0–5 dB. For cochlear hearing loss, the difference ranges from 10–25 dB. A difference of 30 dB or greater indicates neural hearing loss.
Stapedius Muscle Reflex Tone Decay Test
In this test, the stapedius muscle reflex is recorded using an impedance audiometer when the stimulus exceeds the reflex threshold by 10 dB. Normally, the time required for the reflex amplitude to decay by 50% is about 10 seconds. A decay time of less than 5 seconds reflects significant adaptation and suggests retrocochlear pathologies, such as an acoustic neuroma.
Békésy Audiometry
The Békésy audiometer is a device capable of producing both continuous and pulsed pure tones. Based on subject feedback, the machine automatically plots an audiogram with two jagged curves. The outcomes can be categorized into four types:
- Type I: The two curves overlap completely, indicative of normal hearing or conductive hearing loss.
- Type II: At 500–1,000 Hz, the continuous tone curve separates from the pulsed tone curve and declines by 5–20 dB; this reflects loudness recruitment and suggests cochlear pathology.
- Type III: At 125–500 Hz, the continuous tone curve suddenly declines by 40–50 dB; this pattern indicates retrocochlear pathology.
- Type IV: Across frequencies below 500 Hz, the continuous tone curve and pulsed tone curve separate, with a gap greater than in Type II. This pattern is also seen in retrocochlear abnormalities.
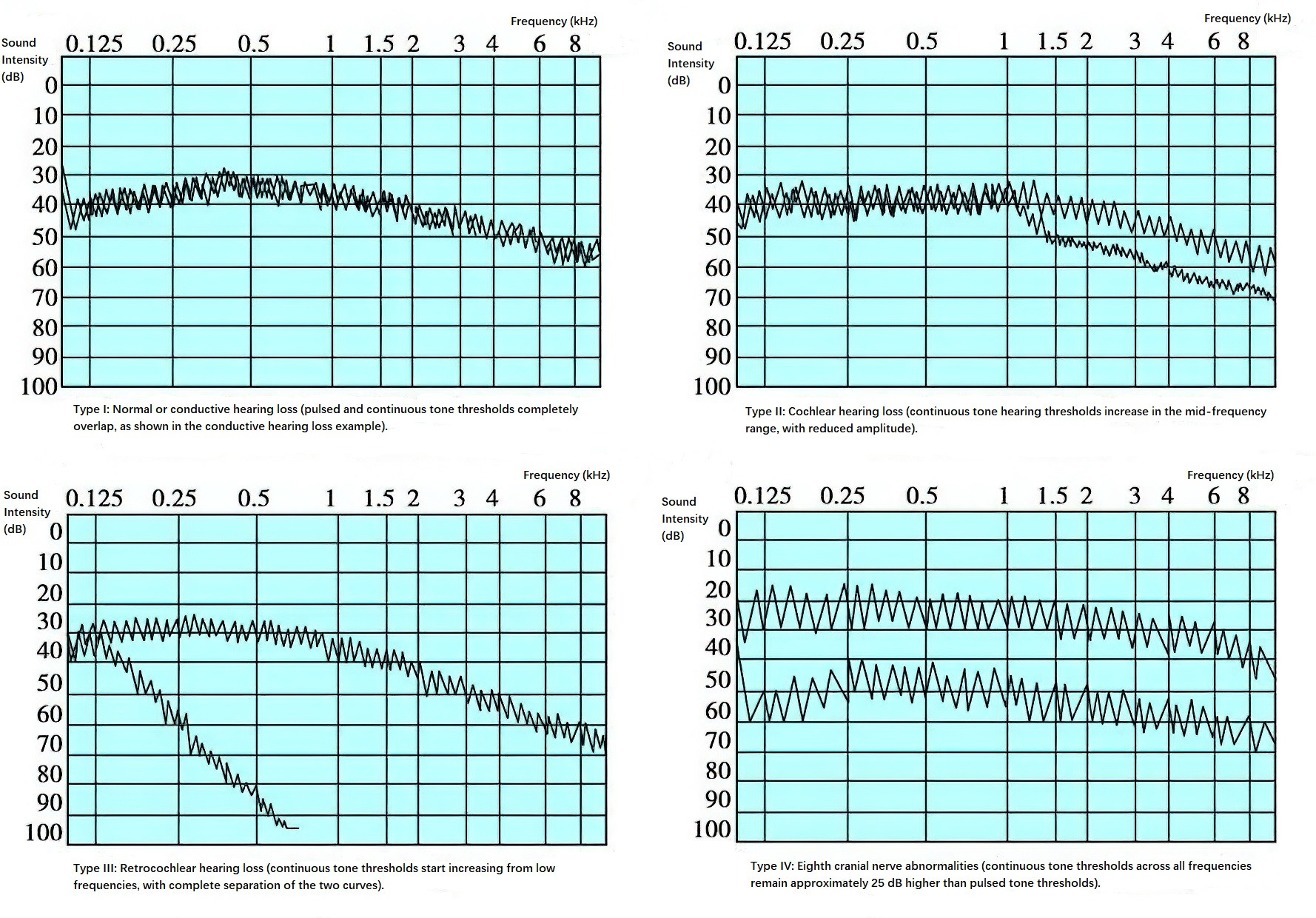
Figure 2 Békésy audiograms
Types III and IV are manifestations of tone decay, which aid in the diagnosis of retrocochlear hearing loss.