Observations include whether the pupils are equal in size, round in shape, centered in position, and whether the edges are smooth. In normal adults, the diameter of the pupil under diffuse natural light typically ranges from 2.5 to 4.0 mm, while it tends to be slightly smaller in infants and elderly individuals. The examination of pupils and their various reflexes is of significant diagnostic value for visual pathways and certain systemic diseases. The details are as follows:
Direct Light Reflex
This refers to the response where the pupil of the tested eye constricts rapidly when light from a flashlight is directed into that eye in a dark room. This reflex requires the involvement of both the afferent and efferent pathways of the pupil reflex in the tested eye.
Indirect (Consensual) Light Reflex
This refers to the response where the pupil of the tested eye constricts rapidly when light is directed into the opposite eye in a dark room. This reflex involves only the efferent pathway of the pupil reflex in the tested eye.
Relative Afferent Pupillary Defect (RAPD)
Also known as Marcus Gunn pupil, this is characterized by the phenomenon where light directed into the affected eye fails to cause pupillary constriction in either eye, whereas light directed into the healthy eye causes bilateral pupillary constriction (the affected eye constricts indirectly). Alternating light between the two eyes at 1-second intervals causes the pupil of the healthy eye to constrict and that of the affected eye to dilate. This sign is particularly useful for diagnosing unilateral retrobulbar optic neuritis, ischemic optic neuropathy, advanced glaucoma, and similar conditions.
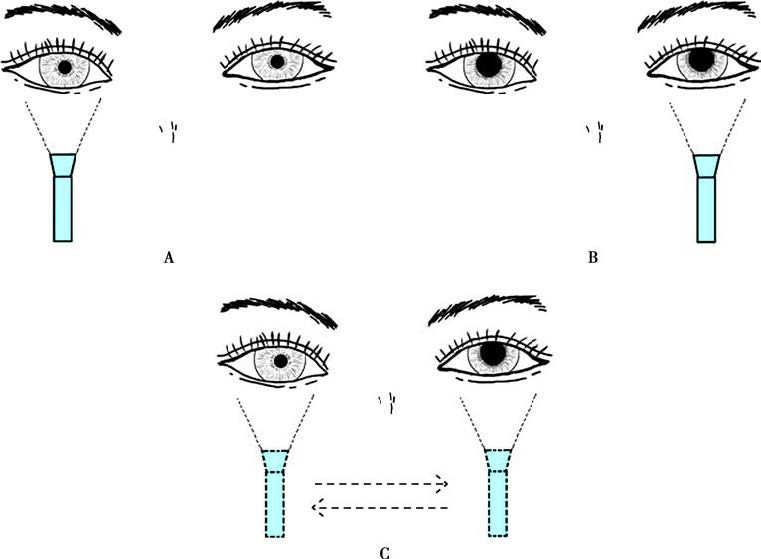
Figure 1 Relative afferent pupillary defect (Left eye as the affected eye)
A. When a flashlight is directed at the right eye, both pupils constrict.
B. When a flashlight is directed at the left eye, neither pupil constricts.
C. Alternating every 1 second, illumination of the healthy eye causes pupillary constriction, while illumination of the affected eye causes pupillary dilation.
Accommodation Reflex
The patient is asked to first focus on a distant object and then immediately shift focus to their index finger at a distance of 15 cm. The pupils of both eyes constrict in response.
Argyll Robertson Pupil
This is characterized by the absence of the direct light reflex while the accommodation reflex remains intact. This sign is commonly observed in neurosyphilis.
Horner’s Pupil
Also known as paralytic miosis, this involves pupil constriction with normal light reflex and near reflex. It is often accompanied by ptosis, narrowing of the palpebral fissure, enophthalmos, and anhidrosis on the affected side of the forehead. This condition is a typical feature of Horner syndrome.
Adie’s Pupil
Also referred to as a tonic pupil, it presents as unilateral pupillary dilation. In a dark room, the affected pupil slowly contracts upon prolonged exposure to bright light and slowly dilates again after the light is removed. The accommodation reflex is also slow in onset and recovery. The affected pupil responds abnormally to miotic agents. This condition is more common in young or middle-aged women and is often accompanied by absent deep tendon reflexes in the limbs. When associated with segmental anhidrosis and orthostatic hypotension, it is referred to as Adie syndrome.