Adverse Reactions to Blood Transfusion and Their Management
When transfusion indications are strictly followed and transfusion procedures are adhered to, most adverse reactions can be prevented.
Febrile Reactions
Febrile reaction is one of the most common early adverse reactions, occurring in 2%–10% of cases. It typically develops within 15 minutes to 2 hours after the start of transfusion, with body temperature rising to 39–40°C. The reaction primarily manifests as chills, shivering, and high fever, often accompanied by headache, sweating, nausea, vomiting, and flushing of the skin. Symptoms usually subside gradually after 30 minutes to 2 hours. In a small number of severe cases, convulsions, respiratory distress, hypotension, or even coma may occur. Febrile reactions rarely develop during general anesthesia.
Etiology
Immune Reaction
This is common in multiparous women or individuals who have received multiple transfusions. The presence of pre-existing leukocyte or platelet antibodies in the recipient can lead to an antigen-antibody reaction, triggering fever upon subsequent transfusions.
Pyrogens
Contamination of transfusion equipment or blood products with pyrogens such as proteins, dead bacteria, or bacterial metabolic byproducts may lead to febrile reactions when introduced into the body.
Management
The underlying cause should be analyzed first. For mild symptoms, reducing the transfusion rate may suffice, while severe cases usually require stopping the transfusion. Warming measures are beneficial during chills and shivering. In cases of high fever, physical cooling measures and glucocorticoids can be applied. For shivering, intramuscular injection of promethazine (25 mg) or pethidine (50 mg) may be used. Blood cultures can help rule out fever caused by microbial infections.
Prevention
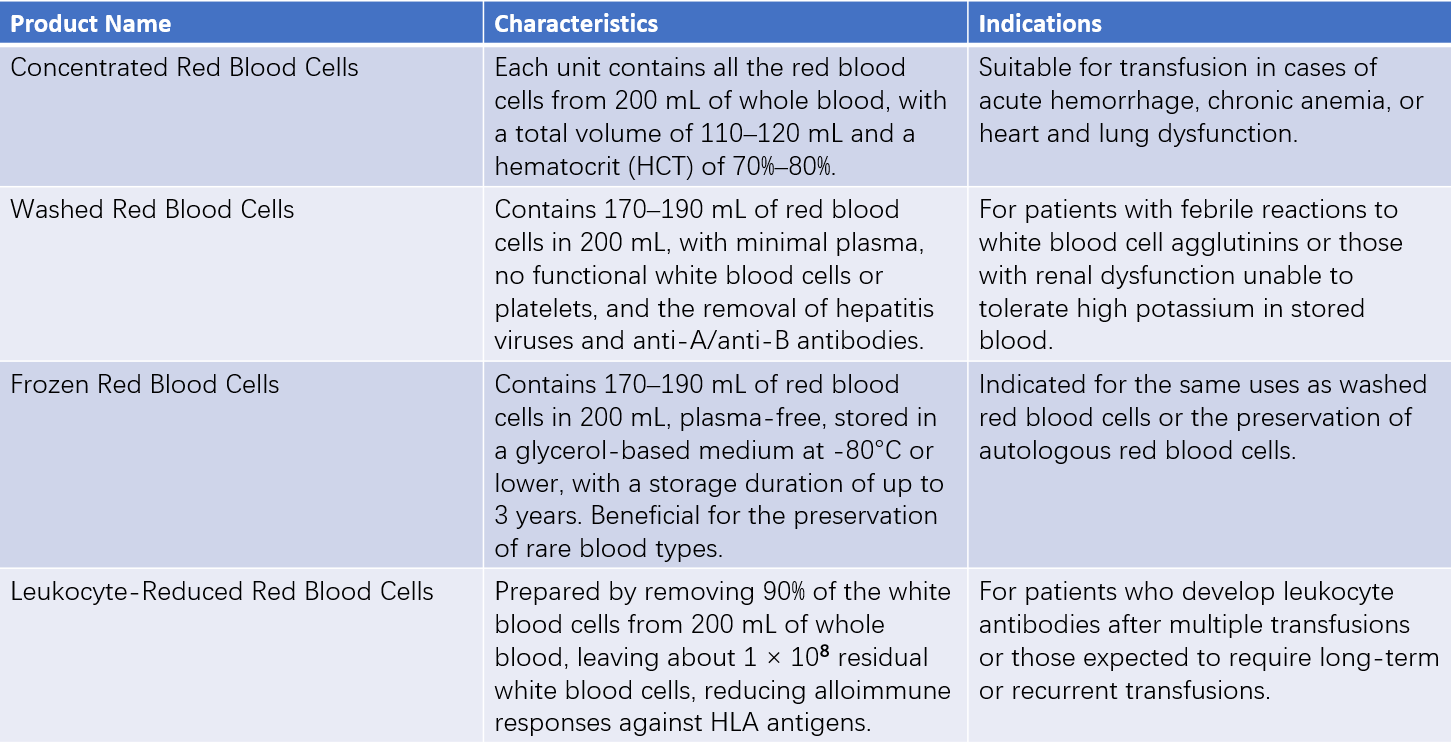
Strict disinfection of transfusion equipment is essential to prevent pyrogen contamination. Leukocyte- and platelet-free blood components, such as washed red blood cells, are recommended for multiparous women or individuals receiving multiple transfusions.
Allergic Reactions
Allergic reactions typically occur within a few minutes after initiating the transfusion, but they can also arise during the transfusion. The incidence is approximately 3%. Symptoms may include localized or generalized skin erythema, itching, or urticaria. In severe cases, anaphylactic shock, loss of consciousness, or even death may occur.
Etiology
Patients with allergic predispositions may react to protein substances present in transfused blood. Similarly, allergic donors may transfer specific antibodies via donated blood, which, upon re-exposure to the allergen, can trigger an allergic reaction in the recipient. The antibodies involved in such cases are often of the IgE subtype.
Repeated transfusion of plasma products may lead to the development of various anti-serum immunoglobulin antibodies, primarily anti-IgA antibodies. Patients with low or deficient IgA levels may exhibit allergic reactions to IgA-containing blood products.
Management
For cases involving limited skin itching or urticaria, temporarily suspending the transfusion and administering oral antihistamines, such as diphenhydramine or promethazine, is warranted while closely monitoring for further symptoms. Severe reactions or cases of anaphylactic shock require immediate cessation of the transfusion. Intramuscular injection of adrenaline (1:1,000, 0.5–1 mL) and/or intravenous glucocorticoid administration is typically employed. Patients with concurrent respiratory distress may require tracheal intubation, puncture, or incision to prevent asphyxia.
Prevention
For patients with a history of allergies, oral administration of antihistamines and intravenous glucocorticoids 30 minutes prior to transfusion is recommended.
Patients with low IgA levels or detectable anti-IgA antibodies should receive IgA-free blood products. If red cell transfusion is necessary, washed red blood cells should be used.
Individuals with known allergic conditions are not suitable as blood donors.
Blood donors should avoid eating within four hours prior to blood donation.
Hemolytic Reactions
Hemolytic reaction is the most severe adverse reaction to blood transfusion. Although its incidence is low, the associated mortality rate is high. Clinical manifestations vary significantly, depending on factors such as the type of incompatible blood group, transfusion rate, volume transfused, and severity of hemolysis. Typical symptoms occur shortly after the transfusion of even a small volume of incompatible blood, manifesting as redness and pain along the transfusion vein, accompanied by chills, high fever, dyspnea, back pain, headache, chest tightness, tachycardia, hypotension, and shock. These symptoms are often followed by hemoglobinuria and hemolytic jaundice. In severe cases, deposition of immune complexes in the glomeruli, disseminated intravascular coagulation (DIC), or reduced renal blood flow due to hypotension may lead to oliguria, anuria, or acute renal failure. Intraoperative patients, being unable to verbalize symptoms, may first exhibit unexplained hypotension and bleeding at the surgical site. Delayed hemolytic transfusion reactions (DHTR) often occur 7 to 14 days after transfusion, presenting as unexplained fever, anemia, jaundice, and hemoglobinuria, though symptoms are generally mild. Recent attention to DHTR highlights its potential to cause systemic inflammatory response syndrome (SIRS), with symptoms such as temperature fluctuations, arrhythmias, leukocyte lysis and reduction, hypertension or decreased peripheral vascular resistance, and, in severe cases, shock, acute respiratory distress syndrome (ARDS), or multi-organ failure.
Etiology
The vast majority of cases result from the transfusion of ABO-incompatible blood, leading to a complement-mediated immune reaction characterized by red blood cell destruction. A sub-type mismatch in group A, Rh incompatibility, or other blood group incompatibilities may also cause hemolysis. Additionally, mismatched donor blood during large-volume transfusion or transfusion from multiple donors in a short period may result in hemolytic reactions.
Non-immune hemolysis may occur occasionally following the infusion of defective red blood cells, such as those subjected to improper storage or transport, preheating at excessive temperatures, or contamination with hypertonic, hypotonic solutions, or substances harmful to red blood cells.
In recipients with autoimmune hemolytic anemia, pre-existing autoantibodies may target transfused red blood cells, triggering a hemolytic reaction.
Management
When hemolytic reaction is suspected, transfusion should be stopped immediately. Verification of the recipient's and donor's names and blood types is necessary. Centrifugation of venous blood and observation of pink plasma provide evidence of hemolysis. Additional diagnostic findings include positive urine occult blood and hemoglobinuria. Blood samples from the donor bag and pre- and post-transfusion samples from the recipient should be tested for blood typing, crossmatching, bacterial smears, and cultures to identify the cause of hemolysis.
Management includes:
- Anti-shock Therapy: Expanding blood volume and correcting hypovolemic shock are essential. Fresh type-matched blood, concentrated platelets, coagulation factors, or glucocorticoids may be administered to control hemolytic anemia.
- Renal Function Protection: Alkalinization of urine with 5% sodium bicarbonate solution (250 mL) helps dissolve hemoglobin crystals and prevents renal tubule obstruction. Once blood volume and urine output return to normal levels, diuretics such as mannitol may be used to expedite the excretion of free hemoglobin. Hemodialysis may be required for oliguria, anuria, azotemia, or hyperkalemia.
- DIC Management: In cases of DIC, prompt correction is necessary.
- Plasmapheresis: This treatment may be utilized to remove abnormal red blood cells and harmful antigen-antibody complexes from the patient's circulatory system.
Prevention
Rigorous implementation of transfusion verification protocols is required.
Procedures should abide by established guidelines to identify defective red blood cell products whenever possible. If preheating of blood is necessary, temperatures must remain strictly below 37°C.
Type-matched transfusion is recommended in non-urgent situations.
Bacterial Contamination Reaction
The clinical manifestations of bacterial contamination reactions depend on the type, virulence, and quantity of bacterial contamination in the transfused product. Mild cases typically present with febrile reactions, while severe cases may progress to septic shock. Without timely intervention, multi-organ failure can occur, resulting in a high mortality rate.
Etiology
Failure to maintain aseptic conditions during blood collection, storage, or transfusion is a major cause of contamination.
Management
Transfusion should be immediately discontinued, and blood from the donor bag should be centrifuged. The plasma and cellular components should undergo bacterial smear, staining, and culture for testing.
Aggressive anti-infective and anti-shock therapies are essential.
Prevention
Strict adherence to aseptic principles is necessary during all stages of blood collection, storage, and transfusion.
Regular inspection of blood during storage and prior to transfusion is important. Suspicious signs, such as discoloration, turbidity, or increased gas production, indicate potential contamination and render the product unsuitable for use.
Circulatory Overload
Circulatory overload is commonly observed in elderly individuals, infants, and patients with cardiac dysfunction or hypoproteinemia. Excessive transfusion volume or overly rapid transfusion rate can cause acute heart failure and pulmonary edema. Clinical manifestations include sudden onset of tachycardia, rapid breathing, cyanosis, or coughing up blood-tinged frothy sputum during or after transfusion. Additional signs include distended neck veins, elevated venous pressure, and significant pulmonary wet rales observed upon auscultation. Chest X-rays reveal evidence of pulmonary edema.
Etiology
Rapid transfusion increases blood volume in a short period, exceeding the heart's capacity to handle the load.
Pre-existing cardiac dysfunction weakens the capacity to tolerate increased blood volume.
Diminished pulmonary function or hypoproteinemia reduces the ability to manage increased blood volume.
Management
Transfusion discontinuation is necessary. Oxygen therapy, along with administration of inotropic agents and diuretics, can help reduce circulatory overload and remove excess fluid.
Prevention
Strict control of transfusion rate and volume is essential for at-risk individuals. For patients with severe anemia, transfusion of concentrated red blood cells is advisable.
Transfusion-Related Acute Lung Injury (TRALI)
TRALI is unrelated to factors such as age, gender, or underlying diseases. The mechanism involves leukocyte agglutinins or human leukocyte antigen (HLA)-specific antibodies present in donor plasma. Clinically, TRALI is difficult to distinguish from non-transfusion-related conditions such as pulmonary infections, aspiration pneumonia, or toxin absorption leading to acute respiratory distress syndrome (ARDS). TRALI manifests as acute respiratory distress, severe bilateral pulmonary edema, and hypoxemia, sometimes accompanied by fever and hypotension. These symptoms typically occur within 1–6 hours after transfusion. Diagnosis requires exclusion of cardiogenic respiratory distress. With effective treatments such as intubation, oxygen therapy, and mechanical ventilation, clinical and physiological improvements are usually observed within 48–96 hours. Chest X-rays typically show resolution of pulmonary infiltrates within 1–4 days, although a small proportion of cases may persist for up to 7 days. Preventive measures involve avoiding the use of plasma from donors who have undergone multiple pregnancies in the production of blood products.
Transfusion-Associated Graft Versus Host Disease (T-GVHD)
T-GVHD occurs when immunologically active lymphocytes from a transfusion are introduced into a severely immunocompromised recipient. The transfused lymphocytes act as grafts, proliferating and reacting against the recipient's tissues. Clinical manifestations include fever, rash, hepatitis, diarrhea, bone marrow suppression, and infection. Disease progression can lead to death. There is currently no effective treatment for T-GVHD, with a mortality rate exceeding 90%. Emphasis is placed on prevention. Blood products intended for patients undergoing bone marrow transplantation, chemotherapy, or radiotherapy should be irradiated using gamma rays or other methods to eliminate immunologically active lymphocytes.
Disease Transmission
Blood transfusion can transmit both viral and bacterial diseases. Viruses include Epstein-Barr virus, cytomegalovirus, hepatitis viruses, human immunodeficiency virus (HIV), and human T-cell leukemia viruses type I and II (HTLV-I, HTLV-II). Examples of bacterial diseases include brucellosis. Other transmissible diseases include syphilis and malaria.
Preventive measures include:
- Strict adherence to transfusion indications.
- Rigorous donor medical examinations.
- Implementation of effective viral inactivation techniques.
- Increased emphasis on the use of autologous blood transfusion.
Immunosuppression
Blood transfusion can lead to nonspecific immunosuppression and antigen-specific immune suppression in recipients. This can increase the rate of postoperative infections and promote tumor growth, metastasis, or recurrence. The extent of immunosuppression caused by blood transfusion is associated with the volume and composition of the transfused blood.