Ossification of the posterior longitudinal ligament (OPLL) refers to a condition where the abnormal proliferation and ossification of the posterior longitudinal ligament in the cervical spine results in reduced spinal canal volume, leading to spinal cord compression and dysfunction of the limbs.
Etiology and Pathology
The etiology of OPLL remains unclear. It is more common in individuals of Asian descent and is associated with genetic, metabolic, or traumatic factors. Ossification of the posterior longitudinal ligament may grow along the longitudinal axis or into the spinal canal. When it progresses to a level that compresses the spinal cord, symptoms and signs appear, which are similar to those of cervical spinal stenosis or myelopathy-type cervical spondylosis. OPLL has the highest incidence in the cervical spine, followed by the thoracic and lumbar spine.
Clinical Manifestations
The onset of this disease commonly occurs in individuals aged 50 to 60 years, with a higher prevalence in men compared to women. Patients often report neck and head pain, sensory abnormalities, or limb dysfunction. The most typical symptom is gait instability, while dysfunction of bladder and bowel control may occur in advanced stages. The condition tends to progress over a long duration, with symptoms of limb and urinary dysfunction gradually worsening. During clinical examination, varying degrees of sensory disturbances may be observed in the upper limbs or all four limbs, along with reduced muscle strength in the limbs and increased muscle tone in the lower limbs. Hyperreflexia is often present, and in severe cases, knee or ankle clonus may be positive. Hoffmann's sign or Babinski's sign may also be positive.
Imaging Examinations
Cervical CT and MRI play essential roles in the diagnosis of OPLL. On lateral X-ray images, CT scans, or two-dimensional reconstructions, dense ossific areas can be observed posterior to the vertebral bodies. The spinal cord may appear compressed and flattened. Based on the extent and morphology of ligament ossification, OPLL can be classified into four types:
- Continuous Type: Ossification spans across two or more segments.
- Segmental Type: Ossification is confined to a single vertebral segment.
- Intermittent Type: Discontinuous ossifications appear across multiple segments.
- Mixed Type: A combination of two or more of the above types in the same individual.
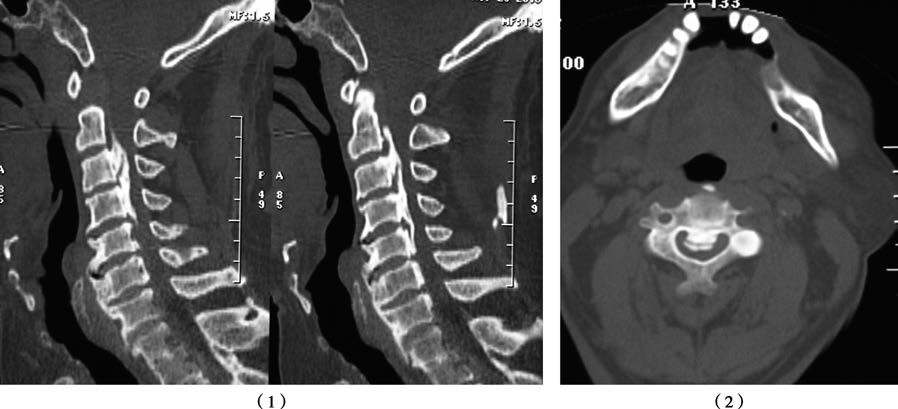
Figure 1 CT results of OPLL in the cervical spine
Sagittal reconstruction (1) and axial images (2) reveal hyperdense, strip-like ossification lesions behind the vertebral bodies, characterized by a broad base and protruding free edges resembling a hill.
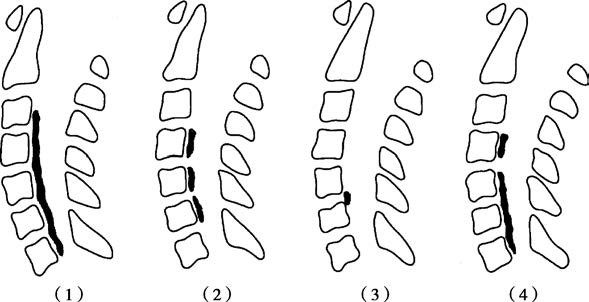
Figure 2 Types of OPLL in the cervical spine
(1) Continuous Type (2) Intermittent Type (3) Segmental Type (4) Mixed Type
Treatment
Non-Surgical Treatment
In cases with mild symptoms, such as minor limb pain or numbness that does not affect work or daily life, non-surgical therapies are recommended. These include rest, the use of oral anti-inflammatory and analgesic medications, and physical therapy.
Surgical Treatment
When significant spinal cord compression symptoms are present, surgical intervention becomes necessary. Surgical approaches include posterior surgery, anterior surgery, or a combined anterior-posterior approach, depending on the type of lesion.