Lateral humeral epicondylitis refers to a chronic inflammatory injury at the origin of the common extensor tendon. It was first observed among tennis players, leading to its alternate name, "tennis elbow."
Etiology and Pathology
Chronic overuse involving repetitive forearm pronation or supination, passive stretching of the extensor muscles (as seen with actions such as gripping with a fist or wrist flexion), and active contraction of the extensor muscles (e.g., wrist extension) generates significant tension at the origin of the common extensor tendon on the lateral epicondyle of the humerus. Prolonged and repetitive engagement in such movements may result in chronic injuries to this area. Occupations and activities that require repetitive forceful wrist movements, such as tennis, badminton, ping pong, or professions like machining work, cooking, and domestic chores, often lead to this injury. In a minority of cases, middle-aged to elderly individuals with weak and deconditioned muscles may develop lateral humeral epicondylitis even after a short period of lifting heavy objects, despite not regularly engaging in physical or sports activities.
The primary pathological change in lateral humeral epicondylitis involves chronic inflammatory injury. The extent of inflammation varies among patients. Some individuals experience localized inflammation primarily in the area of the tip of the lateral epicondyle, manifesting as fasciitis or periostitis. Others may have inflammation extending between the lateral epicondyle of the humerus and the radial head, involving myofasciitis or synovitis of the humeroradial joint.
Clinical Manifestations
Patients typically present with pain on the lateral side of the elbow, which is exacerbated during forceful gripping or wrist extension, resulting in difficulty holding objects. In severe cases, simple daily tasks such as wringing out a towel or sweeping may become challenging. Upon examination, localized and sharp tenderness is present over the lateral epicondyle, the radial head, or the region between them. There are no inflammatory changes in the overlying skin, and joint mobility of the elbow is generally unaffected.
The forearm musculature can be assessed using the extensor stretch test (Mills Test): this is performed with the elbow extended, the hand clenched into a fist, the wrist flexed, and the forearm pronated. Pain on the lateral aspect of the elbow during this maneuver is considered a positive result. In some cases, the pain may also radiate to the mid-upper region of the extensor muscles of the forearm.
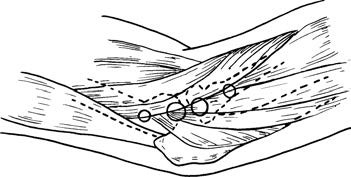
Figure 1 Tender locations associated with lateral humeral epicondylitis
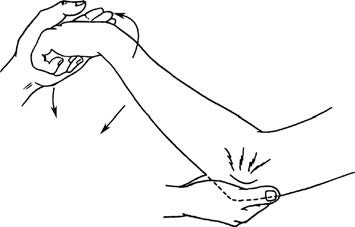
Figure 2 Forearm extensor stretch test (Mills test)
Treatment
Non-surgical treatment is effective for the vast majority of patients.
Limiting wrist joint movements that heavily involve gripping and wrist extension is considered fundamental for treatment and prevention of recurrence.
Injection therapy can be employed by administering a mixture of 1 ml of prednisolone acetate or compound betamethasone injection solution and 1–2 ml of 2% lidocaine into the point of tenderness. This often provides good short-term relief.
Athletes who cannot cease training are advised to reduce the intensity of their activities. Additionally, wrapping an elastic protective strap around the extensor muscle area just below the radial head can help reduce traction stress at the tendon origin.
For patients experiencing persistent pain unresponsive to non-surgical treatments, surgical options may include release and debridement of the origin of the common extensor tendon, excision of neurovascular compression bundles, or arthroscopic surgical interventions.