Supinator syndrome refers to a condition in which the deep branch of the radial nerve (posterior interosseous nerve) is compressed near the tendinous arch of the supinator muscle, primarily leading to dysfunction of the extensor muscles in the forearm.
Anatomical Overview
The supinator muscle originates from the posterolateral surface of the proximal ulna and extends externally, downward, and anteriorly to insert on the lateral surface of the upper radius. It consists of two layers, superficial and deep. The deep branch of the radial nerve passes between these two layers of the supinator muscle. The proximal border of the superficial layer forms a tough tendinous structure known as the tendinous arch of the supinator muscle, where the deep branch of the radial nerve is prone to compression.
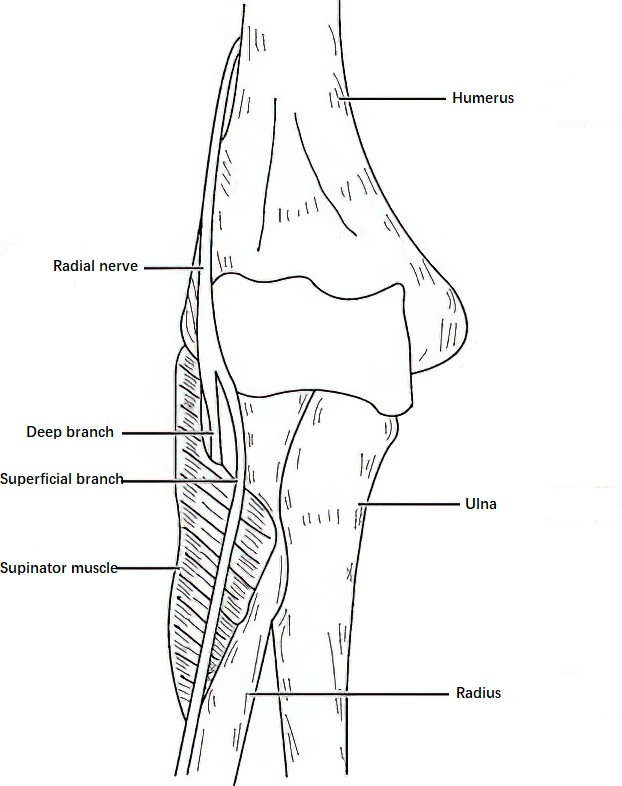
Figure 1 Relationship between the deep branch of radial nerve and the supinator muscle
Etiology
Overuse of the forearm extensor muscles, commonly seen in manual laborers, keyboard operators, or certain athletes, may cause chronic traumatic inflammation of the supinator muscle and lead to hypertrophy, adhesions, or scarring at the tendinous arch. Additionally, non-infectious inflammation due to rheumatoid arthritis can also contribute to these changes. Benign space-occupying lesions near the supinator muscle, such as ganglion cysts or lipomas, as well as anatomical abnormalities in the course of the radial nerve through the supinator muscle, can lead to excessive pressure on the nerve, resulting in functional impairment.
Clinical Features
Incomplete paralysis of muscles innervated by the deep branch of the radial nerve is commonly observed. This includes impaired ability to abduct and extend the thumb and inability to actively extend the metacarpophalangeal joints of the second to fifth fingers. Supination of the forearm may be only slightly affected. The wrist joint can still be actively extended (as the radial wrist extensors are not innervated by the deep branch of the radial nerve), but the wrist tends to deviate towards the radial side. No sensory disturbances are present in the region of the anatomical snuffbox. Electrophysiological studies often reveal denervation changes in the affected muscles and a reduction in motor conduction velocity of the radial nerve in the forearm, while sensory conduction velocity remains normal.
Treatment
Once the diagnosis is confirmed, surgical exploration of the nerve is performed. This involves releasing compression by incising the tendinous arch of the supinator muscle, removing compressive lesions, and performing neurolysis if necessary. Postoperative recovery of deep branch radial nerve function is generally favorable.