Carpal tunnel syndrome is a condition characterized by a set of symptoms and signs resulting from compression of the median nerve within the carpal tunnel. It is the most common type of peripheral nerve entrapment syndrome.
Anatomical Overview
The carpal tunnel is a bony-fibrous canal formed by the carpal bones as the floor and lateral walls, with the flexor retinaculum as the roof. Within the carpal tunnel are the tendon of the flexor pollicis longus, the tendons of the flexor digitorum superficialis and profundus (for digits 2–4), and the median nerve. The median nerve is the most superficial structure, located between the transverse carpal ligament and the other tendons. The flexor pollicis longus tendon is surrounded by the radial synovial sheath, while the remaining tendons are enclosed by the ulnar synovial sheath. During wrist flexion, the median nerve undergoes compression, which intensifies when gripping tightly with the hand.
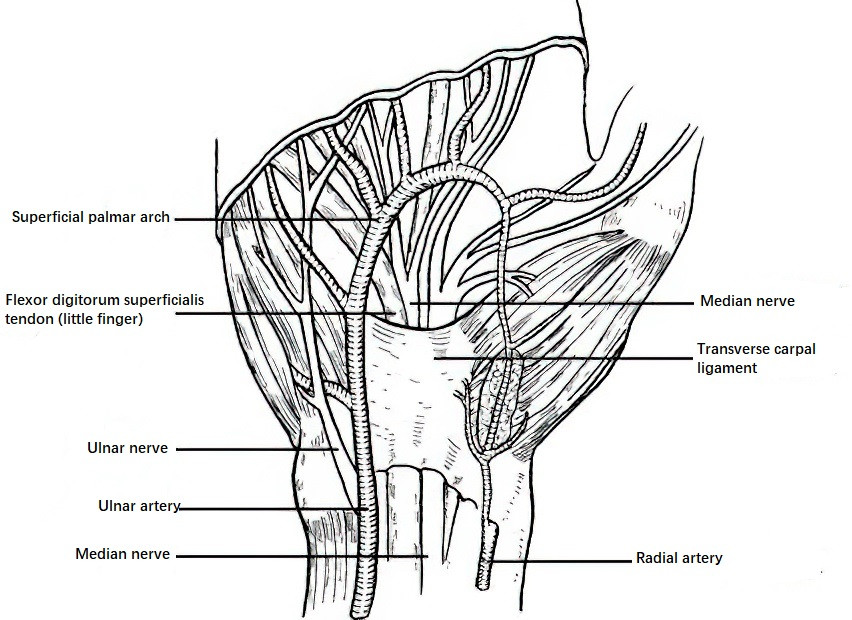
Figure 1 Anatomical relationships at the transverse carpal ligament
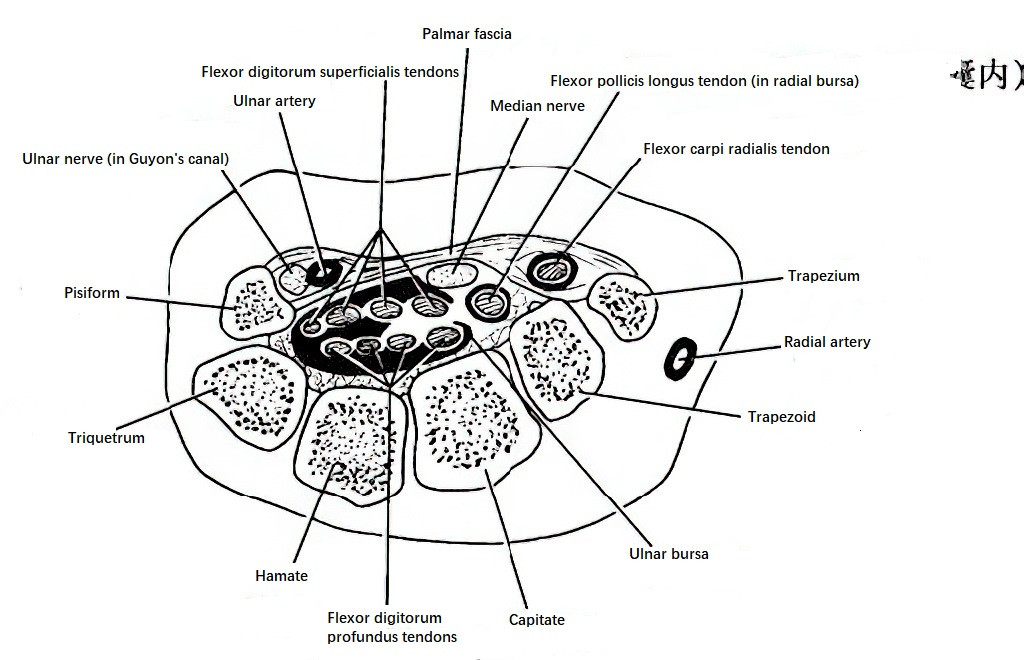
Figure 2 Cross-section of the carpal tunnel
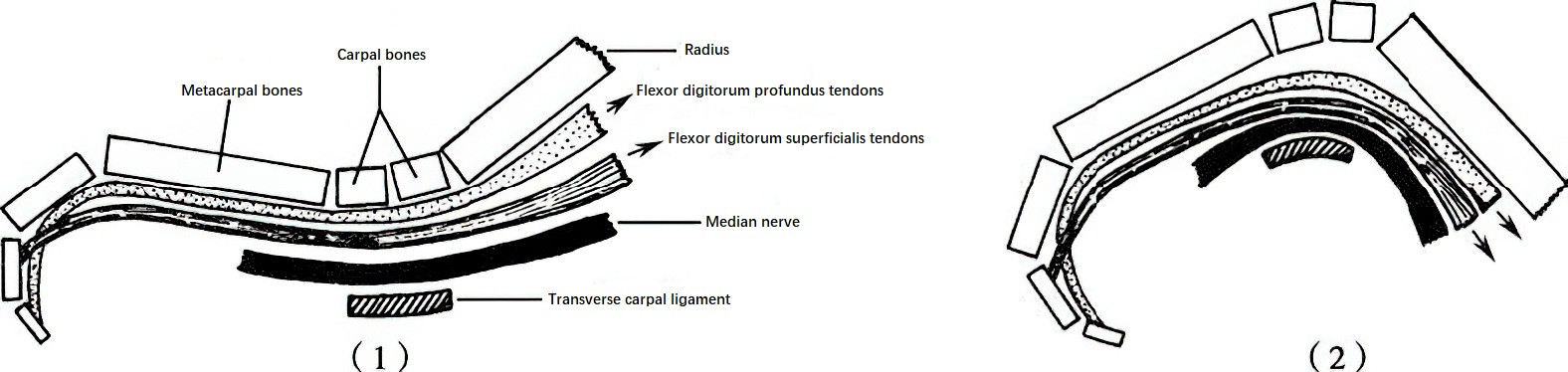
Figure 3 Effect of wrist movements on the median nerve
(1) Dorsiflexion
(2) Palmar flexion
Etiology
External Compression: Compression from the surface of the wrist is rare due to the dense and firm structure of the transverse carpal ligament.
Reduction of Tunnel Volume
The transverse carpal ligament may thicken due to endocrine conditions (such as acromegaly or myxedema) or scarring after trauma. Fractures or dislocations of the wrist (e.g., distal radius fractures, carpal bone fractures, or perilunate dislocations) can cause protrusion of the posterior or lateral walls of the tunnel, leading to narrowing of the carpal tunnel.
Increase in Tunnel Contents or Volume
Conditions such as tendon sheath cysts, neurofibromas, lipomas, and organized hematomas after trauma, as well as synovitis, low-lying muscle bellies of the flexor digitorum muscles, or hypertrophied lumbrical muscles, can increase the contents within the tunnel. This can lead to compression or irritation of the median nerve.
Occupational Factors
Professions that involve repetitive and forceful use of the wrist, such as carpenters or chefs, can be associated with repeated rapid fluctuations in carpal tunnel pressure. For example, the pressure within the carpal tunnel during excessive wrist flexion can increase to 100 times that of the neutral position, while during excessive wrist extension, the pressure can increase to 300 times. These changes in pressure can contribute to chronic damage to the median nerve.
Clinical Presentation
This condition is more common in middle-aged women, with men typically having an occupational history. Bilateral involvement occurs in more than 30% of cases, with up to 90% of bilateral cases occurring in postmenopausal women.
Patients commonly report numbness or pain in the tips of the radial three fingers, along with weakened grip strength, particularly affecting the middle finger. Symptoms are often most severe at night or in the early morning but can be alleviated by adjusting the position of the wrist. Pain may occasionally radiate to the forearm.
Physical Examination
Sensory hypersensitivity or dullness may be observed in the thumb, index finger, and middle finger. Thenar muscle atrophy may develop, leading to weakened thumb opposition. A positive Tinel’s sign over the median nerve at the wrist is often observed. The Phalen test, performed by flexing the elbows, raising the forearms, and simultaneously flexing both wrists to 90° for one minute, can provoke symptoms of median nerve irritation. This test has a sensitivity rate of approximately 70%. In cases of inflammation or masses within the carpal tunnel, local swelling, tenderness, or palpation of the edges of a mass may be noted.

Figure 4 Phalen's test (Wrist flexion test)
Electrophysiological Examination
Findings may demonstrate nerve damage, including electromyographic abnormalities of the thenar muscles and slowing of median nerve conduction velocity between the wrist and fingers.
Differential Diagnosis
Carpal tunnel syndrome should primarily be distinguished from other causes of chronic median nerve lesions proximal to the wrist. A common differential diagnosis is the radicular form of cervical spondylosis. In such cases, it is important to note that the symptoms of carpal tunnel syndrome are limited to areas distal to the wrist, while radicular cervical spondylosis may also affect forearm flexor muscles. Additionally, the Phalen test and Tinel’s sign are usually negative in cervical spondylosis. Electrophysiological results can further differentiate the two conditions.
Treatment
Non-Surgical Treatment
In the early stages, immobilization of the wrist in a neutral position may be employed along with pharmacological or physical therapy. Injection of prednisolone acetate into the carpal tunnel may provide good results but is contraindicated in cases of tumors or suppurative inflammation. Care should be taken to avoid injecting the medication directly into the nerve, as this can cause chemical inflammation due to corticosteroid crystal accumulation, worsening the symptoms.
Surgical Treatment
Surgical resection is indicated for conditions such as synovial cysts within the carpal tunnel, chronic synovitis of long duration, benign tumors, or ectopic muscle bellies. In cases of tunnel narrowing caused by thickening of the walls, decompression by cutting the transverse carpal ligament may be performed. If the median nerve is found to be hardened or locally enlarged during the operation, epineurotomy or scar excision between nerve fascicles can be performed as part of neurolysis.