Acetabular fractures are intra-articular fractures of the largest load-bearing joint in the human body, accounting for 10% of pelvic injuries. They are primarily caused by high-energy trauma and are more common in young and middle-aged individuals. Low-energy trauma is more frequently observed in elderly individuals, with an increasing incidence. The acetabulum is a hemispherical deep socket located in the lower-middle part of the hip bone, inclined anteriorly, downward, and outward. It is composed of the anterior column (iliopubic column), anterior wall, posterior column (ilioischial column), and posterior wall. The anterior column descends obliquely from the anterior portion of the iliac crest to the pubic symphysis, while the posterior column extends from the plane of the greater sciatic notch to the ischial tuberosity, forming the roof of the acetabulum. Common mechanisms of acetabular fractures include:
- Direct force applied to the greater trochanter and transmitted along the femoral neck axis to the acetabulum.
- Force applied to the foot, knee, or femoral head, transmitted along the lower limb axis to the acetabulum.
- Force applied to the iliolumbar region, resulting not only in pelvic fractures but also possibly involving the acetabulum.
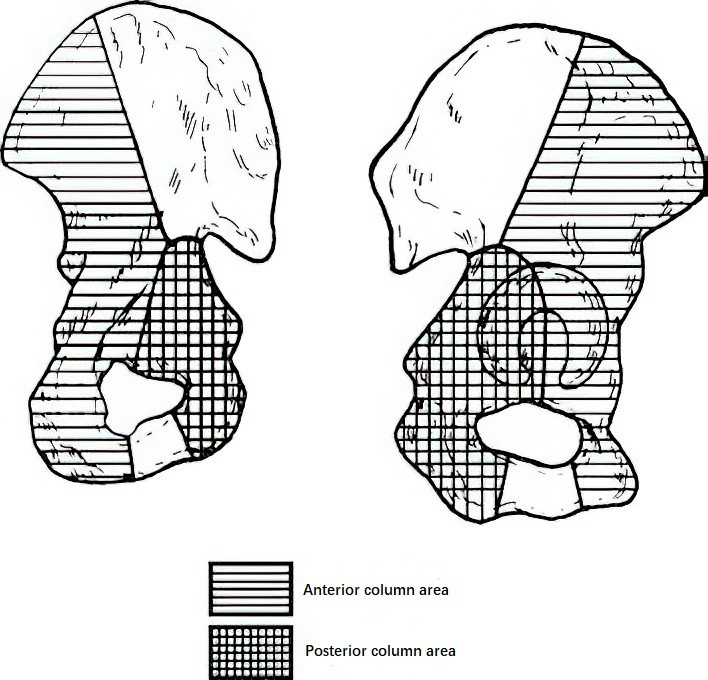
Figure 1 Diagram of Acetabular Anatomy
The nature, direction, and position of the lower limb during trauma can lead to different types of fractures. In severe cases, the femoral head may perforate the acetabulum and enter the pelvic cavity, causing central hip dislocation.
Fracture Classification
Several classification systems exist for acetabular fractures, such as the Letournel-Judet classification, Marvin-Tile classification, and AO/OTA classification. The Letournel-Judet classification is commonly used and is based on alterations in anatomical structures, identifying 10 types of fractures.
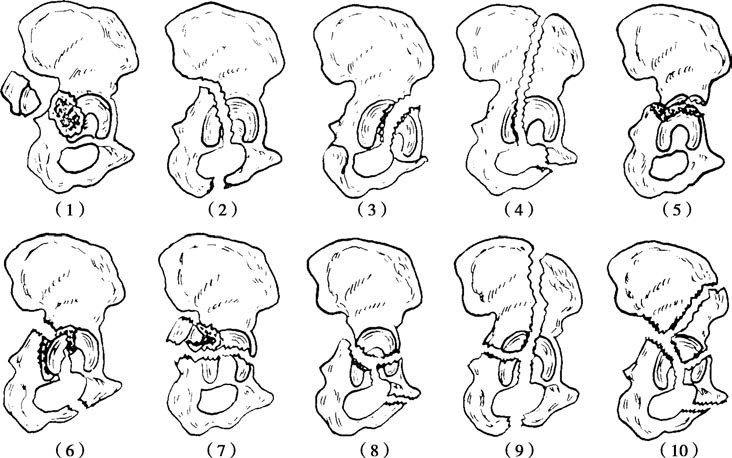
Figure 2 Schematic representation of Letournel-Judet classification
1, Posterior wall fracture
2, Posterior column fracture
3, Anterior wall fracture
4, Anterior column fracture
5, Transverse fracture
6, Posterior column with posterior wall fracture
7, Transverse fracture with posterior wall fracture
8, T-shaped fracture
9, Anterior column with posterior hemitransverse fracture
10, Both-column fracture
Simple Fractures
These involve a single column or wall of the acetabulum and include five categories:
- Posterior wall fracture
- Posterior column fracture
- Anterior wall fracture
- Anterior column fracture
- Transverse fracture
Complex Fractures
These involve at least two simple fracture types and include five categories:
- T-shaped fracture
- Posterior column with posterior wall fracture
- Transverse fracture with posterior wall fracture
- Anterior column with posterior half transverse fracture
- Both-column fracture
Treatment
As an intra-articular fracture of the body's primary load-bearing joint, all treatment approaches follow the principles of intra-articular fracture management: achieving anatomic reduction, stable fixation, and early functional rehabilitation whenever possible. Acetabular fractures with displacement are ideally treated surgically, though specific treatment plans depend on a variety of factors.
Conservative Treatment
Conservative treatment mainly involves bed rest and traction. Indications include:
- Non-displaced fractures or displacement <2 mm.
- Severe osteoporosis.
- Presence of local or systemic infections.
- Surgical contraindications, such as coexisting systemic diseases precluding surgery.
- Satisfactory and relatively stable closed reduction of the fracture.
Surgical Treatment
Indications
Surgical indications include:
- Acetabular fractures with displacement >2 mm within 3 weeks of the injury, provided no surgical contraindications exist.
- Emergency surgery is indicated in the following situations:
- Irreducible hip dislocation.
- Unstable hip joint after attempted reduction.
- Hip dislocation complicated by femoral head fracture.
- Progressive worsening of associated nerve injuries.
- Concurrent vascular injuries.
- Open acetabular fractures.
Time to Surgery
Given the frequent association of acetabular fractures with pelvic fractures and/or other injuries, significant bleeding, and the complexity of exposure for fracture reduction, surgery usually requires experienced surgeons. The optimal timing is typically 4–7 days post-injury.
Preoperative Preparation
Preparation primarily includes bowel preparation and the preparation of the affected limb, with preoperative traction applied to the affected side.
Surgical Approaches and Techniques
The choice of surgical approach generally depends on the type of acetabular fracture. Common approaches include:
- The posterior Kocher-Langenbeck approach, suitable for posterior wall fractures, posterior column fractures, transverse fractures with posterior wall involvement, and most T-shaped fractures.
- The anterior ilioinguinal approach, appropriate for anterior column fractures, anterior wall fractures, and most both-column fractures.
- The iliofemoral approach or a combined anterior-posterior approach.
For fractures of the anterior column or wall of the acetabulum, modern approaches such as the modified Stoppa approach or the pararectus approach are also frequently utilized.
Surgical techniques include open reduction with fixation using reconstruction plates or W-shaped acetabular plates, fixation with hollow screws, and total hip arthroplasty where appropriate.