In most cases, metatarsal fractures result from direct trauma, such as impact from heavy objects or compression injuries like being run over by a vehicle. In fewer cases, fractures may occur due to chronic overuse injuries, such as those caused by long-distance running or prolonged marching, leading to stress fractures of the second or third metatarsal shaft. Metatarsal fractures account for 2.4% of all fractures in adults and 23.3% of foot fractures. Among the five metatarsals, the first metatarsal is the largest and has a lower likelihood of fracturing. Fractures are most commonly seen in the second to fourth metatarsals. The base of the fifth metatarsal, being composed mostly of cancellous bone, is prone to fractures caused by forceful contraction of the peroneus brevis muscle. Isolated fractures of the fifth metatarsal base can be treated with bracing or cast immobilization for 4 to 6 weeks, after which functional rehabilitation may begin.
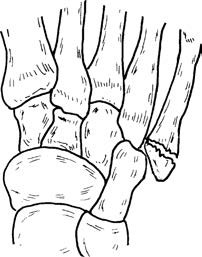
Figure 1 Fracture of the fifth metatarsal base
Metatarsal fractures can occur at the metatarsal base, shaft, or neck. Fractures of the metatarsal base often result in downward and posterior displacement of the distal fragment and may compress or injure the plantar arterial arch. If there is concurrent damage to the dorsalis pedis artery or insufficient compensatory blood flow, necrosis of the forefoot may occur. Emergency closed reduction and cast immobilization are required in such cases. If closed reduction fails, internal fixation can be performed by inserting an intramedullary pin through the sub-head region of the metatarsal to cross the fracture site and into the tarsal bones.
Metatarsal shaft fractures present with different patterns such as transverse, oblique, or comminuted fractures depending on the magnitude and direction of the applied force. Fractures of the second to fourth metatarsal shafts that are simple and non-displaced usually do not require special treatment, and activity with weight-bearing may resume after 3 to 4 weeks of rest. Displaced fractures involving multiple metatarsal shafts may first undergo trial closed reduction. If this reduction is unsuccessful, open reduction is pursued with fixation using an intramedullary pin inserted through the sub-head region of the metatarsals for 4 to 6 weeks.
Fractures of the metatarsal neck often involve downward and posterior displacement of the distal fragment, causing drooping of the metatarsal head, which affects the normal weight-bearing mechanics of the foot and can result in pain. Closed reduction is typically attempted first. If this is not successful, open reduction is performed, followed by internal fixation with crossed Kirschner wires. The wires are usually removed 4 to 6 weeks after fixation. Weight-bearing walking can resume once solid bone healing is achieved.

Figure 2 Fracture of the metatarsal neck