Anatomical Overview
The fibrous layer of the ankle joint capsule is thickened to form ligaments, which are primarily organized into three groups:
- Medial Collateral Ligament: Also known as the deltoid ligament, it is the strongest ligament of the ankle joint. Its main function is to prevent ankle eversion.
- Lateral Collateral Ligament: Originating from the lateral malleolus, it comprises three bundles inserting respectively on the anterolateral talus, lateral calcaneus, and posterior calcaneus. This is the weakest ligamentous structure in the ankle.
- Inferior Tibiofibular Ligament: Also known as the transverse tibiofibular ligament, it consists of anterior and posterior bands that tightly connect the distal tibia and fibula. It deepens the anterior and posterior aspects of the ankle mortise and provides joint stability.
Damage to the medial collateral ligament may result in lateral instability of the ankle joint, while injury to the lateral collateral ligament may lead to multidirectional ankle instability.
Etiology
An ankle sprain may occur during activities such as stepping down stairs or walking on uneven surfaces, particularly when the ankle is in plantar flexion. Inversion or eversion forces may excessively stretch the ankle ligaments, leading to partial tears, complete rupture, elongation, avulsion fractures, or subluxation/dislocation of the ankle joint or the inferior tibiofibular syndesmosis. Inadequate healing of acute ligament injuries can result in ligamentous laxity and recurrent injuries, contributing to chronic ankle instability.
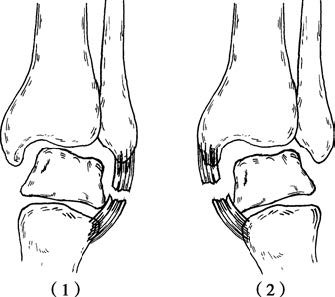
Figure 1 Ligament injuries of the ankle
(1) Lateral ligament injury due to inversion force
(2) Medial ligament injury due to eversion force
Clinical Manifestations and Diagnosis
Following an ankle sprain, pain, swelling, and subcutaneous ecchymosis typically occur, with increased pain during movement. Physical examination may reveal localized tenderness. When pressure is applied while the ankle is in plantar flexion and the foot is inverted or everted, pain intensifies, suggesting ligamentous injury.
Diagnosis of partial tears, laxity, or complete rupture may sometimes be challenging. An anteroposterior X-ray taken with the ankle in extreme inversion under compression may reveal significant widening of the lateral joint space, indicating complete lateral ligament rupture. A lateral X-ray may show anterior subluxation of the talus. Avulsion fractures may also be seen on standard anteroposterior and lateral ankle X-rays.
Treatment
In the acute phase, cold compresses are used immediately to reduce local bleeding and swelling. After 48 hours, localized physical therapy may be initiated to promote tissue healing.
For partial ligament injuries or ligamentous laxity, immobilization is performed with the ankle in 90° dorsiflexion and in extreme inversion (for medial ligament injuries) or eversion (for lateral ligament injuries), using a plaster cast or wide adhesive tape or bandage for 2 to 3 weeks.
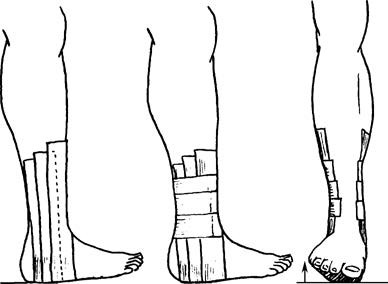
Figure 2 External fixation for ankle ligament injuries
In cases of complete ligament rupture with joint instability, or when accompanied by small avulsion fractures, immobilization with a cast for 4 to 6 weeks may be considered. If a fracture fragment enters the joint space, open reduction and fixation of the fragment may be required, followed by casting for 3 to 4 weeks.
For chronic ankle instability caused by recurrent injuries and ligamentous laxity, autologous tendon transfer or allograft tendon reconstruction may be used to restore joint stability. Over time, chronic instability may lead to ankle dislocation and degenerative changes of the articular cartilage, resulting in osteoarthritis. Surgical intervention may be indicated if conservative treatment proves ineffective.