Distal femur fractures include supracondylar fractures, intercondylar fractures, and condylar fractures involving the articular surface of the distal femur. These injuries account for approximately 0.92% of all fractures. Due to the presence of joint capsules, ligaments, muscles, and tendons around the femoral condyles, fracture fragments are prone to displacement as a result of traction from these structures. Additionally, there may be associated injuries to the popliteal vessels, nerves, and surrounding soft tissues.
Anatomical Overview
The distal femur includes the femoral condyles and the supracondylar region. The medial and lateral condyles form the articular surface of the distal femur. The posterior aspect of the distal femur serves as the origin of the medial and lateral heads of the gastrocnemius muscle. The femoral condyles articulate with the corresponding tibial plateaus. The lateral aspect of the lateral condyle serves as the origin of the lateral collateral ligament. The medial condyle is larger than the lateral condyle; its medial surface is concave and gives rise to the medial collateral ligament distally. The adductor tubercle, located at the superior aspect of the medial condyle, serves as the insertion point for the adductor magnus muscle.
Classification and Mechanism of Injury
Supracondylar fractures refer to fractures that occur between the femoral condyles and the metaphyseal region of the distal femoral shaft, representing the transition between cortical and cancellous bone. Most cases are caused by high-energy trauma such as falls from a height. The distal fragment may be displaced posteriorly due to traction by the hamstring and gastrocnemius muscles, posing a risk of vascular and nerve injury. Femoral condylar fractures may involve the articular surface or disrupt the weight-bearing axis of the lower limb, often requiring open reduction and internal fixation. Intercondylar fractures of the femur are often referred to as T-shaped fractures.
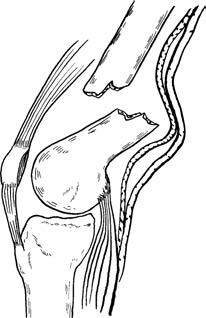
Figure 1 Typical deformity in distal femur fracture
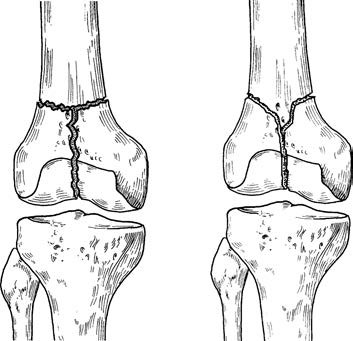
Figure 2 Intercondylar fracture of the femur (T-shaped fracture)
Clinical Presentation and Diagnosis
Swelling, deformity, and tenderness are typically present around the knee joint and distal femur. Abnormal movement and crepitus can be detected at the fracture site. In cases of poor lower limb perfusion or weak dorsalis pedis pulses, vascular injury should be suspected. Doppler ultrasound is useful for assessing potential popliteal artery damage, and angiography may be performed when necessary. Standard anteroposterior and lateral X-rays of the distal femur are commonly obtained. For fractures caused by high-energy trauma such as traffic accidents, a pelvic X-ray should also be acquired to avoid missed diagnoses. Since distal femur fractures are frequently associated with deep vein thrombosis in the lower extremities, Doppler ultrasound is routinely performed.
Treatment
Non-surgical treatment includes closed reduction, skeletal traction, and cylindrical plaster cast immobilization. However, these methods often result in prolonged bed rest, increased difficulty in care, and higher risk of complications. As a result, they are now used less frequently.
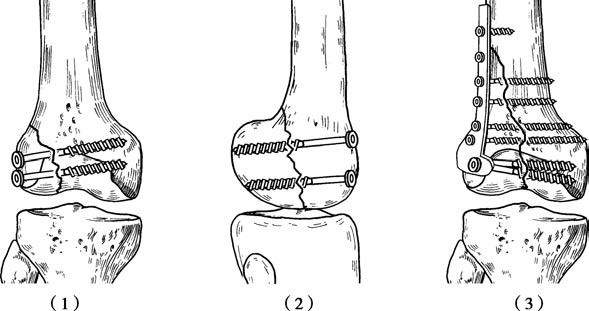
Figure 3 Internal fixation with cancellous screws and a buttress plate
(1), (2): Cancellous bone screw fixation
(3): Buttress plate fixation
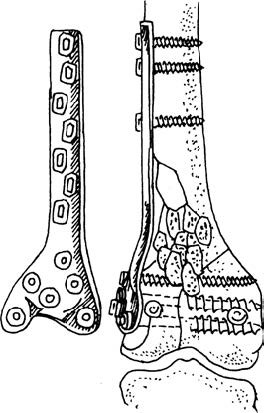
Figure 4 Internal fixation with anatomical plate for the femoral condyle
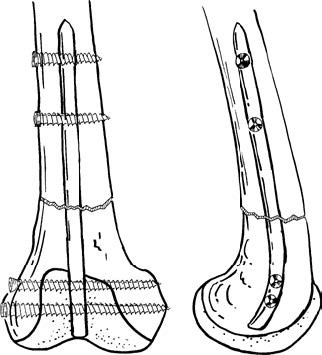
Figure 5 Internal fixation with retrograde locked intramedullary nail for the distal femur
Surgical treatment aims to achieve anatomical reduction, stable internal fixation, and early rehabilitation. The vast majority of distal femur fractures require surgical intervention. Common internal fixation techniques include:
- Cancellous bone screws combined with a buttress plate
- Anatomical plate for the femoral condyle
- Retrograde locked intramedullary nail for the distal femur