Anatomical Overview
The elbow joint is composed of the distal humerus, the olecranon of the ulna, the radial head, the joint capsule, and the medial and lateral collateral ligaments. It primarily facilitates flexion and extension movements, along with slight ulnar and radial deviation. Among the shoulder, elbow, hip, and knee, the elbow joint ranks second in likelihood of dislocation.
Etiology and Classification
Trauma is the main cause of elbow dislocations. Dislocations can be classified as anterior, posterior, or lateral. A posterior dislocation typically occurs when the elbow is in a semi-flexed position during a fall, with the palm striking the ground. The force is transmitted proximally along the radius and ulna, creating a lever effect at the olecranon. This causes a tear in the anterior joint capsule, displacing the radius and ulna posteriorly from the humerus. Lateral dislocations can occur when valgus or varus stress is applied to the elbow joint, causing medial or lateral displacement, respectively. An anterior dislocation may result when the elbow joint is flexed at the time of trauma, and posterior force displaces the radius and ulna anteriorly relative to the humerus. Elbow dislocations often lead to tears in the medial and lateral collateral ligaments, resulting in joint instability.
Clinical Presentation and Diagnosis
After an upper limb injury, patients typically present with elbow pain, swelling, and restricted movement. Physical examination reveals a posterior prominence deformity of the elbow, with the forearm in a semi-flexed position and elastic fixation. A hollow or depression may be palpated posteriorly, where the elbow joint normally resides, and the normal triangular relationship of bony landmarks around the elbow is altered. These findings suggest the possibility of a posterior elbow dislocation. Anteroposterior and lateral X-rays of the elbow can reveal the degree of displacement and assess for accompanying fractures. Lateral dislocations may also involve nerve injuries, necessitating an examination of hand sensation and motor function.
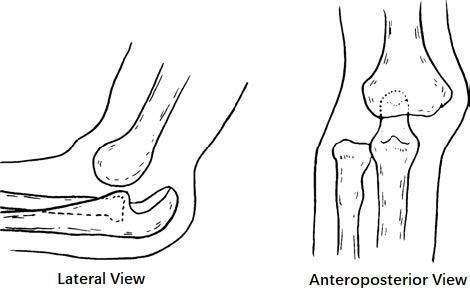
Figure 1 Deformity in posterior elbow dislocation with radial displacement
Treatment
Closed Reduction
Reduction may be performed using a single-person method. Successful reduction is marked by the restoration of normal elbow movement and the reestablishment of the triangular relationship of the bony landmarks. For the single-person cradle reduction method, the patient is seated with the injured limb held by the practitioner. The elbow is flexed, with the practitioner applying traction to the forearm with one hand while using the thumb of the other hand to press on the olecranon to guide it back into position.

Figure 2 Reduction method for posterior elbow dislocation
Immobilization
The elbow is immobilized in 90° of flexion using a long-arm plaster splint or brace. The forearm is suspended in a sling and immobilized for 2–3 weeks. After this period, the patient begins elbow flexion and extension exercises to prevent joint stiffness.
Figure 3 Immobilization with plaster splint after manual reduction
Surgical Treatment
If functional exercises reveal significant elbow instability or an evident tendency for redislocation when the joint is flexed beyond 30°, surgical reconstruction of the elbow ligaments is indicated.