Hallux valgus, commonly referred to as "bunion," is a common forefoot deformity characterized by lateral deviation of the big toe and medial displacement of the first metatarsal.
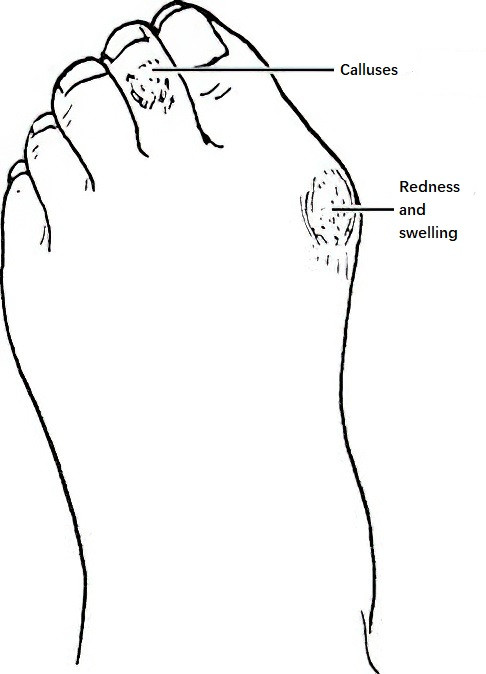
Figure 1 Hallux valgus features
Etiology
The condition is often associated with genetic predisposition and improper footwear. Over 80% of cases have a family history. It is more common in women, with a higher prevalence in those wearing high-heeled shoes. Strong ligaments connect the cuneiform and metatarsal bones of the foot, but the connection between the medial cuneiform and the first metatarsal is relatively weaker. Prolonged standing, excessive walking, or wearing high-heeled or pointed-toe shoes can increase pressure on the medial cuneiform and metatarsal by more than 25%, causing medial displacement of the first metatarsal. This contributes to the collapse of the longitudinal and transverse arches. The toe moves laterally due to the pull of the adductor muscles and the extensor digitorum longus, increasing the angle between the first and second metatarsals.
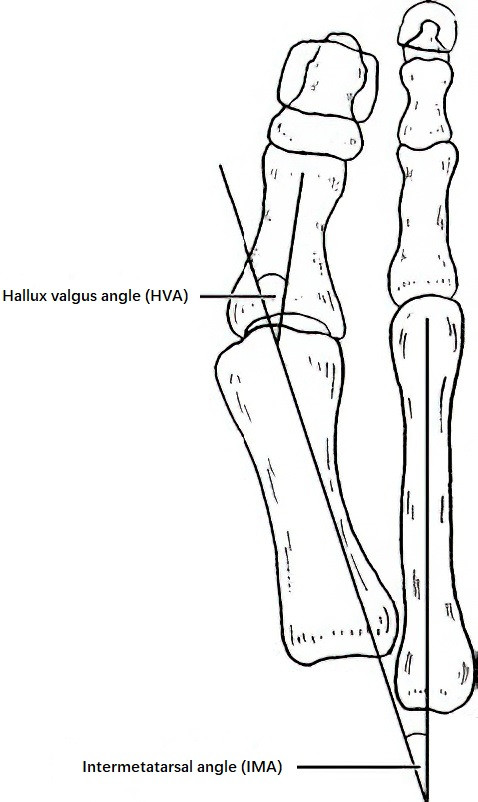
Figure 2 Angles associated with hallux valgus
The medial aspect of the first metatarsal head may develop a bony prominence, and the hallux valgus deformity progressively worsens. The second toe may be displaced dorsally by the big toe, and the interphalangeal joints may become flexed, resulting in hammer toes.
Clinical Manifestations
Hallux valgus is more commonly observed in middle-aged and elderly women and often presents bilaterally. Mild subluxation can occur at the metatarsophalangeal joint of the big toe. The medial joint capsule attachment site may experience pulling stress, leading to the formation of bony prominences. The first metatarsal head, being prominent on the medial side of the foot, often undergoes chronic friction with footwear, causing local skin thickening. A subcutaneous bursa may develop over this site, which, if red, swollen, or inflamed, results in bursitis. Severe cases may lead to osteoarthritis of the metatarsophalangeal joint, resulting in pain. The plantar skin overlying the second and third metatarsal heads may develop calluses due to increased weight-bearing. Similarly, calluses or corns may form on the dorsal skin of the proximal interphalangeal joint of the second toe due to friction with footwear.
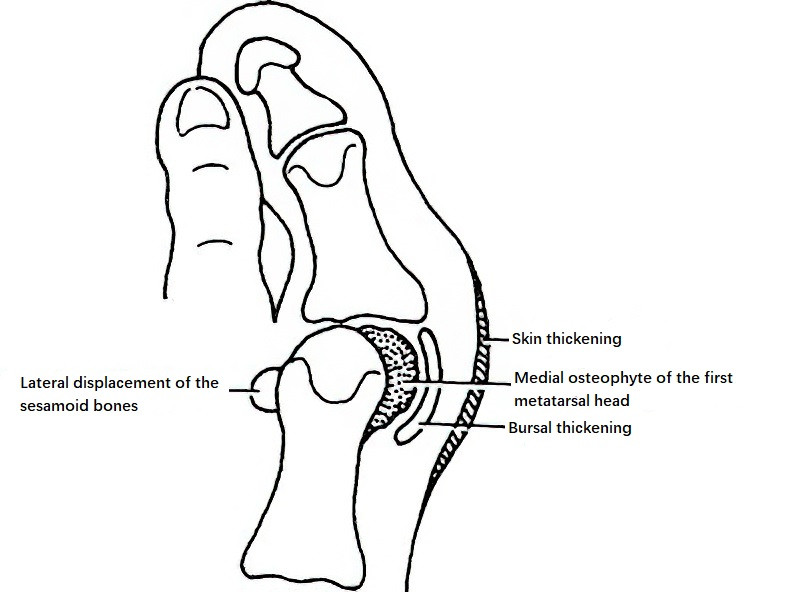
Figure 3 Bursitis and osteophyte formation due to hallux valgus
Imaging Studies
To assess the condition in detail, confirm the diagnosis, and guide treatment, weight-bearing anteroposterior, lateral, and sesamoid axial X-rays of the foot are obtained.
Hallux valgus angle (HVA)
This is the angle between the axes of the first metatarsal and the proximal phalanx of the big toe. It represents the degree of valgus deformity. In normal individuals, the average HVA is 10.1° in men and 10.6° in women. An HVA greater than 15° is considered abnormal.
Intermetatarsal angle (IMA)
This is the angle between the axes of the first and second metatarsals. It reflects the degree of medial displacement of the first metatarsal. In normal individuals, the average IMA is 8.3° in men and 9.9° in women. An IMA greater than 10° is considered abnormal.
Treatment
Conservative Treatment
Conservative measures may be considered for patients with mild deformities and less severe symptoms. Wearing wide-toed shoes can help reduce pressure and friction on the medial side of the toes. Various devices are available to prevent progression of hallux valgus. Silicone toe separators or toe alignment socks can be applied between the first and second toes in mild cases. Orthopedic braces, corrective footwear, or insoles for flat feet can also assist in managing the condition.
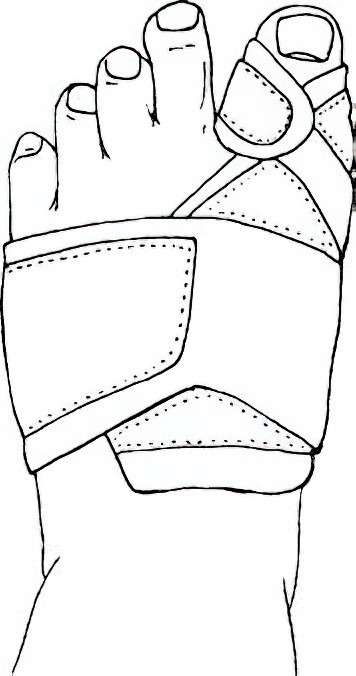
Figure 4 Hallux valgus corrective brace
Surgical Treatment
Surgical intervention may be considered when conservative treatment fails, or in cases of severe pain and deformity. The goals of surgery are to correct the deformity, alleviate pain, and restore a more aesthetically pleasing appearance. Over a hundred surgical techniques for hallux valgus have been reported, each with its advantages and disadvantages. These methods can be broadly categorized into:
- Soft tissue procedures: McBride procedure is a representative example.
- Osteotomy procedures: Techniques like Mayo and Keller osteotomy are less commonly used today.
- Combined soft tissue and osteotomy procedures: These include Chevron osteotomy, Scarf osteotomy, and Akin osteotomy.
Recent studies have reported the clinical application of metatarsophalangeal joint reconstruction, including artificial joint replacement.