Hydrocele refers to an abnormal accumulation of fluid within the tunica vaginalis of the testis and/or the spermatic cord, forming a cystic mass. The condition is classified into testicular hydrocele, funicular hydrocele, testicular and funicular hydrocele, and communicating hydrocele.
Etiology and Classification
Under normal conditions, only a small amount of serous fluid is present in the tunica vaginalis. Hydrocele forms when the balance between secretion and absorption of fluid by the tunica vaginalis is disrupted, leading to excessive secretion or insufficient absorption. Communicating hydrocele is caused by incomplete closure of the processus vaginalis.
Incomplete or aberrant closure of the processus vaginalis at different locations can result in various types of hydroceles:
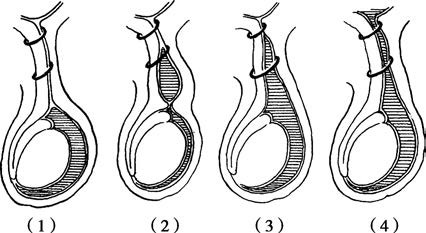
Figure 1 Various types of hydroceles
(1) Testicular hydrocele
(2) Funicular hydrocele
(3) Testicular and funicular hydrocele
(4) Communicating hydrocele
Testicular Hydrocele
The processus vaginalis closes normally, but excessive fluid accumulates within the tunica vaginalis, forming a spherical or oval-shaped hydrocele. It can be primary, with an unknown cause, or secondary, resulting from inflammation, trauma, tumors, or filariasis. In such cases, the fluid may appear turbid, bloody, or chylous. Secondary testicular hydrocele can also occur after surgery for varicocele. Preserving lymphatic vessels during surgery can effectively prevent postoperative hydrocele.
Funicular Hydrocele
Both ends of the processus vaginalis close, but the mid-portion remains patent and contains fluid. This type does not communicate with the abdominal cavity or the testicular tunica vaginalis and is also referred to as a spermatic cyst.
Testicular and Funicular Hydrocele
The processus vaginalis closes at the internal inguinal ring but remains open along the spermatic cord, which communicates with the testicular tunica vaginalis. The mass has a pear-shaped appearance. Although the external inguinal ring expands due to fluid pressure, there is no communication with the abdominal cavity.
Communicating Hydrocele
Incomplete closure of the processus vaginalis results in a hydrocele that communicates with the peritoneal cavity via a small channel. This is also known as a congenital hydrocele. In some cases, intestinal loops or the greater omentum may enter the tunica vaginalis, causing a congenital indirect inguinal hernia.
Clinical Manifestations
Hydroceles most commonly occur on one side and manifest as a cystic mass in the scrotum or inguinal region. They typically grow slowly, are painless, and present a chronic course. Mild cases may be asymptomatic, while severe cases with larger fluid accumulation may cause a feeling of scrotal heaviness, distension, or traction. Large testicular hydroceles may retract the penis into the foreskin, potentially interfering with urination, walking, or daily activities.
Diagnosis and Differential Diagnosis
Testicular hydrocele presents as a spherical or oval-shaped mass with a smooth surface, elastic texture, and cystic feel. Pain is usually absent, and the testis or epididymis is typically not palpable. A positive transillumination test confirms a clear fluid-filled mass; however, if the fluid is purulent, bloody, or chylous, the transillumination test may be negative.
Funicular hydrocele often presents as one or more cystic masses that are elliptical, fusiform, or dumbbell-shaped, located along the spermatic cord. The normal testis and epididymis can be palpated below the mass. When the testis is gently pulled, the hydrocele may move vertically along with it.
Ultrasound typically reveals an anechoic fluid-filled area. In the case of testicular hydrocele, a distinct boundary with the testis is observed. Testicular and funicular hydroceles may present as a pear-shaped mass in the scrotum, while the testis may not be easily palpable. Communicating hydroceles exhibit enlargement of the scrotum in the standing position, with fluid flowing back into the abdominal cavity in the supine position, causing the hydrocele to shrink or disappear. Ultrasound is a reliable diagnostic tool for hydrocele.
Differentiation is necessary between testicular hydrocele, testicular tumors, and indirect inguinal hernias. Testicular tumors present as solid, firm masses with a sensation of heaviness and a negative transillumination test. Indirect inguinal hernias may exhibit intestinal loops or bowel sounds in the affected scrotum, with reducible contents upon lying flat. A cough impulse may be palpable at the internal inguinal ring, and the transillumination test will also be negative.
Treatment
In adults, testicular hydroceles with small amounts of fluid and no symptoms do not require surgical intervention. When the hydrocele is large and symptomatic, excision of the tunica vaginalis followed by eversion (Lord's procedure) is performed. Funicular hydrocele necessitates complete excision of the cyst. Communicating hydroceles are treated by high ligation of the processus vaginalis at the internal inguinal ring.
Congenital hydroceles in infants often resolve spontaneously as the fluid gets absorbed, so surgical treatment is generally deferred. Surgical intervention is suggested only if the condition persists beyond the first year of life.
For secondary testicular hydrocele caused by traumatic hematocele, conservative management is appropriate if there is minimal blood accumulation; however, significant hematoma requires surgical removal of blood clots with meticulous hemostasis. In chylous hydroceles containing microfilariae, diethylcarbamazine therapy is administered alongside eversion of the tunica vaginalis.